

Posterolateral transpedicular approach for ventrally seated cervicothoracic spinal cord lesions: how I do it
- PMID: 36414756
- PMCID: PMC9840581
- DOI: 10.1007/s00701-022-05424-2
Posterolateral transpedicular approach for ventrally seated cervicothoracic spinal cord lesions: how I do it
Abstract
Background: Surgical exposure of lower cervical and upper thoracic intradural extramedullary lesions located along the ventral medulla are among the most complexes to address in spinal surgery, and their surgical removal carries a high risk.
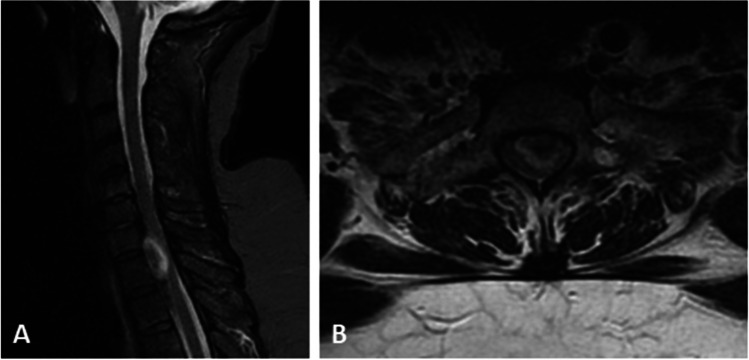
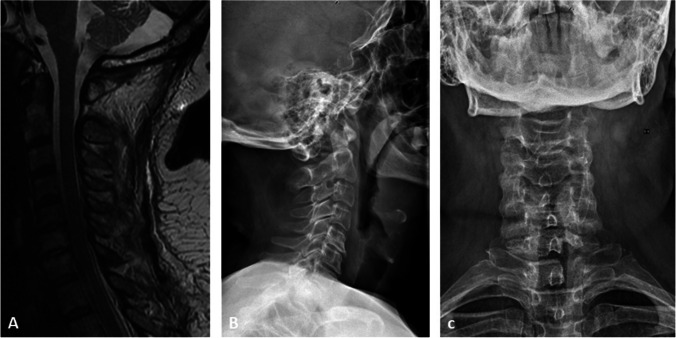
Methods: We describe the surgical steps of a posterolateral transpedicular approach for resection of an intradural extramedullary lesion located anterolaterally at C7-T1 level.
Conclusions: A posterolateral transpedicular approach is a safe and efficient surgical corridor to explore the ventral spinal cord and to have a direct access to lower cervical-upper thoracic lesions without the extensive manipulation of the spinal cord and the spine instability.
Keywords: Cervicothoracic region; Spinal cord tumor; Surgical approach; Transpedicular approach; Ventral spinal lesion.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Zhang J, Tsuzuki N, Hirabayashi S, Saiki K, Fujita K. Surgical anatomy of the nerves and muscles in the posterior cervical spine: a guide for avoiding inadvertent nerve injuries during the posterior approach. Spine (Phila Pa 1976) 2003;28(13):1379–84. doi: 10.1097/01.BRS.0000067095.75764.D3. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
