

Risk factors for the development of premature ventricular complex-induced cardiomyopathy: a systematic review and meta-analysis
- PMID: 36414810
- PMCID: PMC10333144
- DOI: 10.1007/s10840-022-01421-8
Risk factors for the development of premature ventricular complex-induced cardiomyopathy: a systematic review and meta-analysis
Abstract
Background: Premature ventricular complexes (PVCs) are a potentially reversible cause of heart failure. However, the characteristics of patients most likely to develop impaired left ventricular function are unclear. Hence, the objective of this study is to systematically assess risk factors for the development of PVC-induced cardiomyopathy.
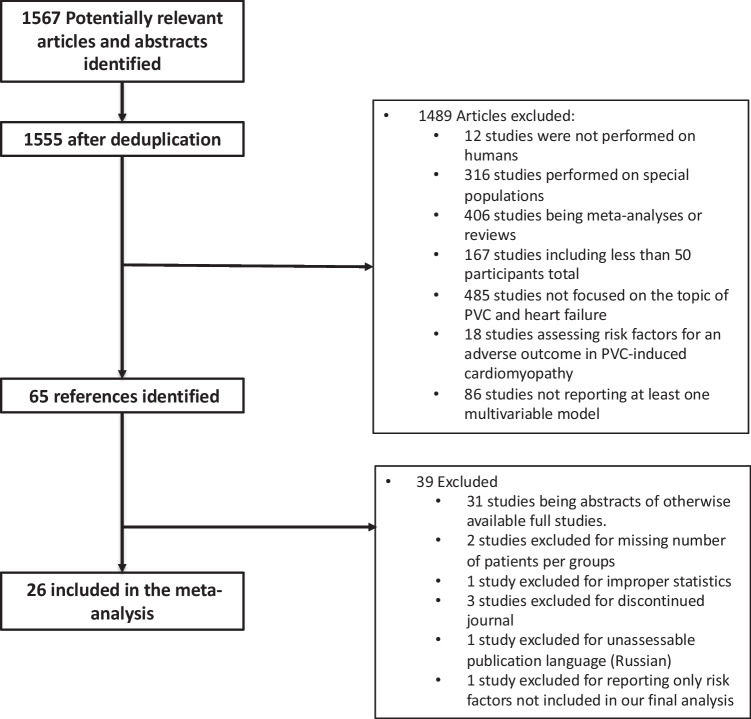
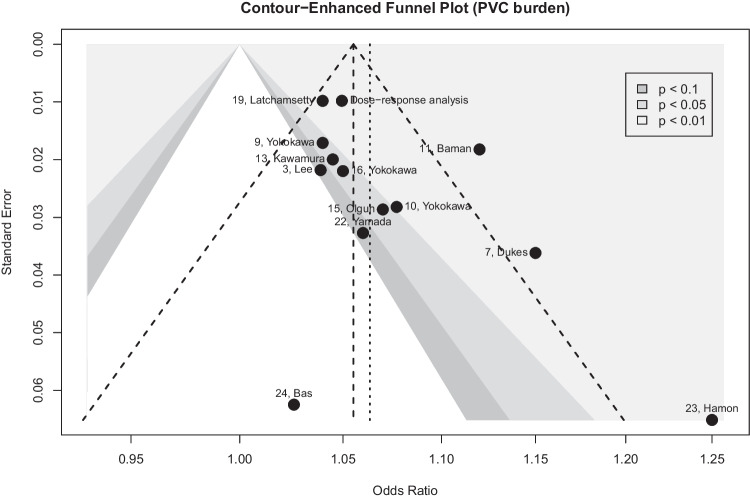
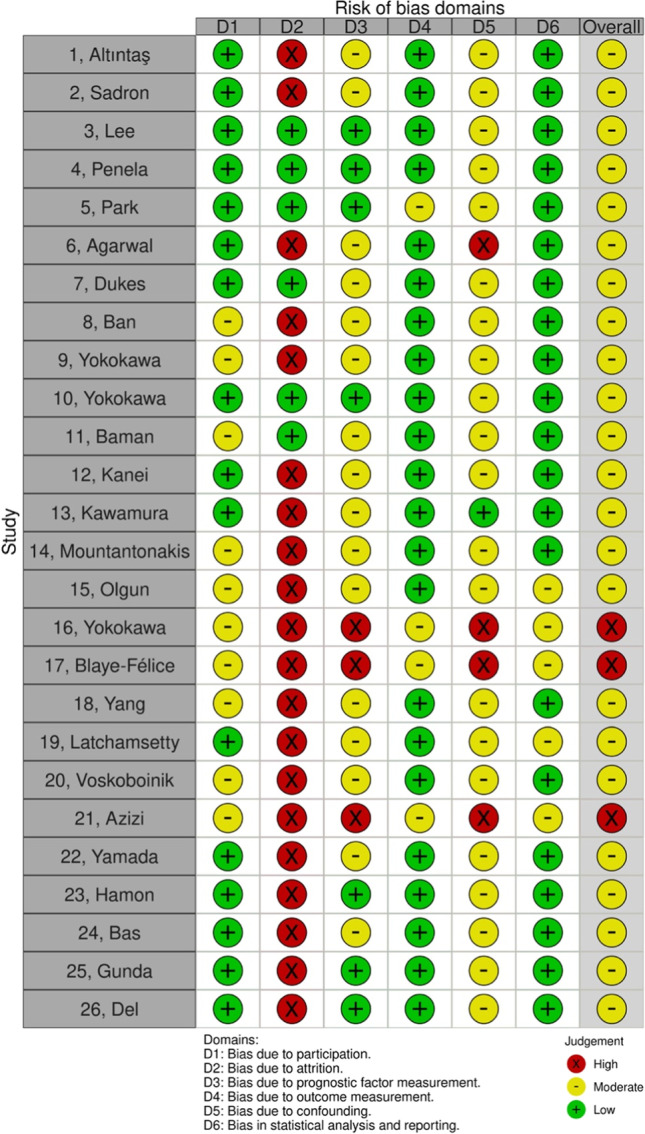
Methods: We performed a structured database search of the scientific literature for studies investigating risk factors for the development of PVC-induced cardiomyopathy (PVC-CM). We investigated the reporting of PVC-CM risk factors (RF) and assessed the comparative association of the different RF using random-effect meta-analysis.
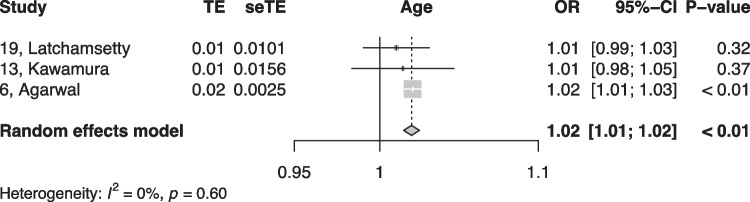
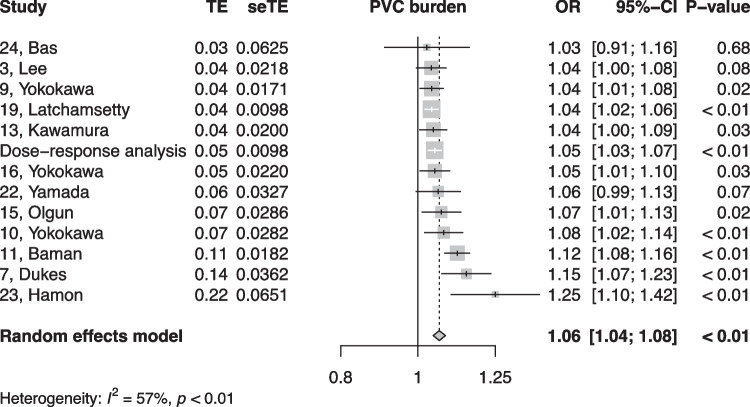
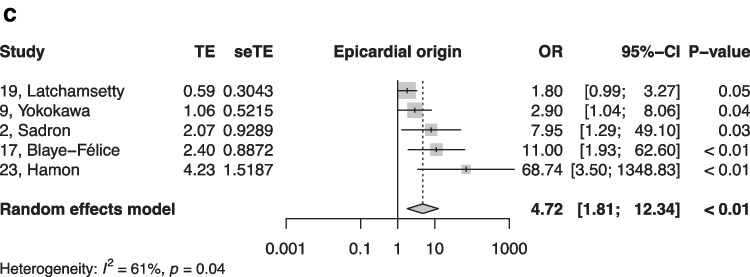
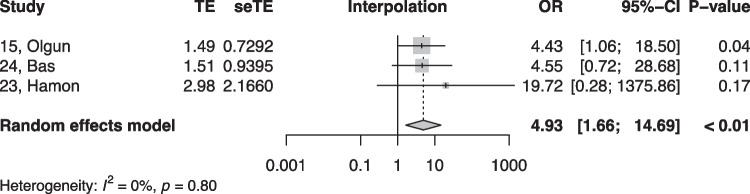
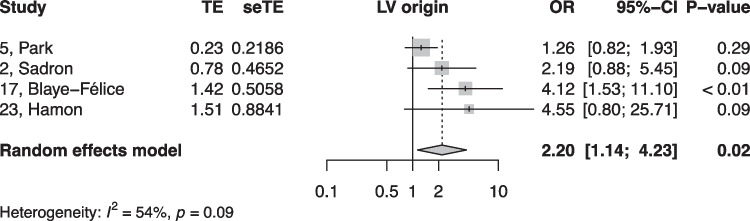
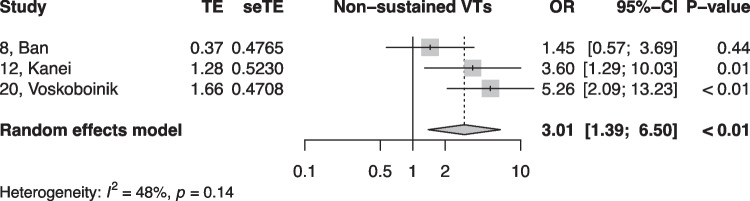
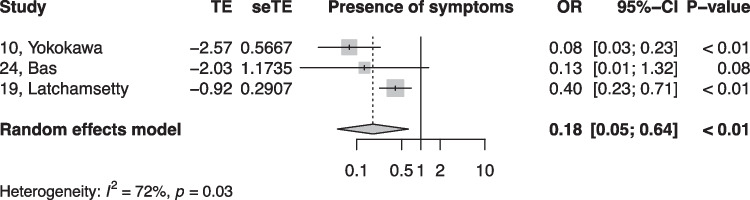
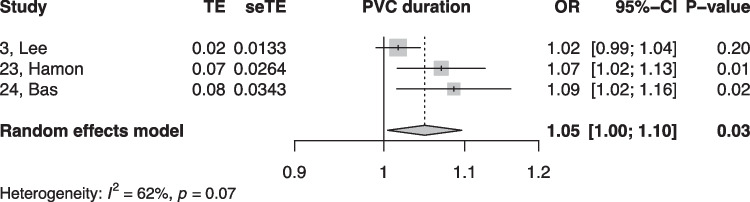
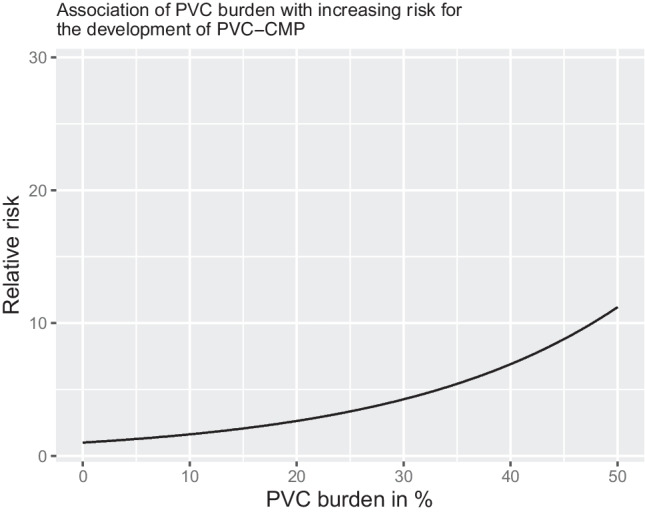
Results: A total of 26 studies (9 prospective and 17 retrospective studies) involving 16,764,641 patients were analyzed (mean age 55 years, 58% women, mean PVC burden 17%). Eleven RF were suitable for quantitative analysis (≥ 3 occurrences in multivariable model assessing a binary change in left ventricular (LV) function). Among these, age (OR 1.02 per increase in the year of age, 95% CI [1.01, 1.02]), the presence of symptoms (OR 0.18, 95% CI [0.05, 0.64]), non-sustained ventricular tachycardias (VT) (OR 3.01, 95% CI [1.39, 6.50]), LV origin (OR 2.20, 95% CI [1.14, 4.23]), epicardial origin (OR 4.72, 95% CI [1.81, 12.34]), the presence of interpolation (OR 4.93, 95% CI [1.66, 14.69]), PVC duration (OR 1.05 per ms increase in QRS-PVC duration [1.004; 1.096]), and PVC burden (OR 1.06, 95% CI [1.04, 1.08]) were all significantly associated with PVC-CM.
Conclusions: In this meta-analysis, the most consistent risk factors for PVC-CM were age, non-sustained VT, LV, epicardial origin, interpolation, and PVC burden, whereas the presence of symptoms significantly reduced the risk. These findings help tailor stringent follow-up of patients presenting with frequent PVCs and normal LV function.
Keywords: Hear failure; PVC-induced cardiomyopathy; Premature ventricular contractions; Ventricular arrhythmias.
© 2022. The Author(s).
Conflict of interest statement
Sven Knecht has received funding of the “Stiftung für Herzschrittmacher und Elektrophysiologie.”
Michael Kühne reports personal fees from Bayer, personal fees from Böhringer Ingelheim, personal fees from Pfizer BMS, personal fees from Daiichi Sankyo, personal fees from Medtronic, personal fees from Biotronik, personal fees from Boston Scientific, personal fees from Johnson & Johnson, personal fees from Roche, grants from Bayer, grants from Pfizer, grants from Boston Scientific, grants from BMS, grants from Biotronik, and grants from Daiichi Sankyo, all outside the submitted work.
Christian Sticherling is a Member of Medtronic Advisory Board Europe and Boston Scientific Advisory Board Europe, received educational grants from Biosense Webster and Biotronik and a research grant from the European Union’s FP7 program and Biosense Webster, and lecture and consulting fees from Abbott, Medtronic, Biosense-Webster, Boston Scientific, Microport, and Biotronik, all outside the submitted work.
Patrick Badertscher has received research funding from the “University of Basel,” the “Stiftung für Herzschrittmacher und Elektrophysiologie,” the “Freiwillige Akademische Gesellschaft Basel,” and Johnson & Johnson, all outside the submitted work and reports personal fees from Abbott.
Jeanne du Fay de Lavallaz has received research funding from the “University of Basel” and from the “Swiss Heart Foundation.”
Henry Huang has received research funding from Medtronic, educational grants from Medtronic, Biotronik, Abbott, and Boston Scientific, and consulting fees from Biosense-Webster and Cardiofocus.
Michael Gold is a consultant to Boston Scientific and Medtronic, as well as on steering committees with Boston Scientific, Abbott, and Medtronic.
Others have nothing to declare.
Figures
References
-
- Bozkurt, B. et al. Current diagnostic and treatment strategies for specific dilated cardiomyopathies: a scientific statement from the American Heart Association. Circulation. 2016; 134: e579–e646 Preprint at 10.1161/CIR.0000000000000455 - PubMed
-
- Takemoto M, et al. Radiofrequency catheter ablation of premature ventricular complexes from right ventricular outflow tract improves left ventricular dilation and clinical status in patients without structural heart disease. J Am Coll Cardiol. 2005;45:1259–1265. doi: 10.1016/j.jacc.2004.12.073. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
