

Effect of Stay-at-Home orders and other COVID-related policies on trauma hospitalization rates and disparities in the USA: a statewide time-series analysis
- PMID: 36414998
- PMCID: PMC9680127
- DOI: 10.1186/s40621-022-00409-2
Effect of Stay-at-Home orders and other COVID-related policies on trauma hospitalization rates and disparities in the USA: a statewide time-series analysis
Abstract
Background: To combat the coronavirus pandemic, states implemented several public health policies to reduce infection and transmission. Increasing evidence suggests that these prevention strategies also have had a profound impact on non-COVID healthcare utilization. The goal of this study was to determine the impact of a statewide Stay-at-Home order and other COVID-related policies on trauma hospitalizations, stratified by race/ethnicity, age, and sex.
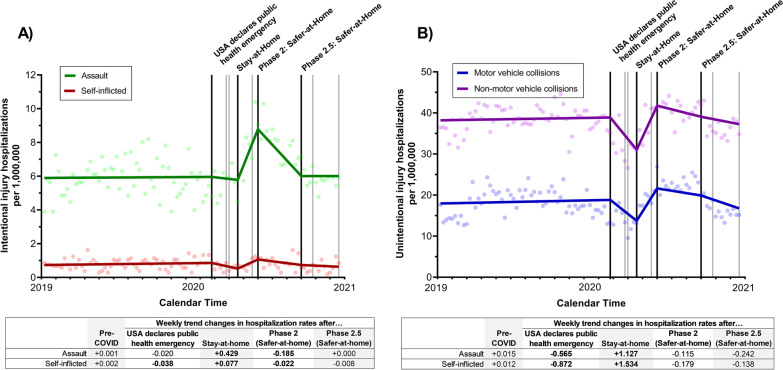
Methods: We used the North Carolina Trauma Registry, a statewide registry of trauma hospitalizations for 18 hospitals across North Carolina, including all North Carolina trauma centers, to calculate weekly rates of assault, self-inflicted, unintentional motor vehicle collision (MVC), and other unintentional injury hospitalizations between January 1, 2019, and December 31, 2020. Interrupted time-series design and segmented linear regression were used to estimate changes in hospitalization rates after several COVID-related executive orders, overall and stratified by race/ethnicity, age, and sex. Changes in hospitalization rates were assessed after 1) USA declaration of a public health emergency; 2) North Carolina statewide Stay-at-Home order; 3) Stay-at-Home order lifted with restrictions (Phase 2: Safer-at-Home); and 4) further lifting of restrictions (Phase 2.5: Safer-at-Home).
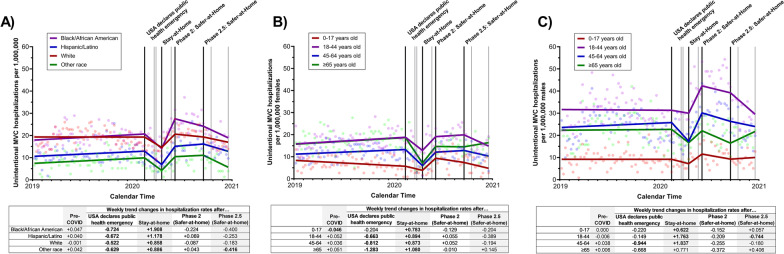
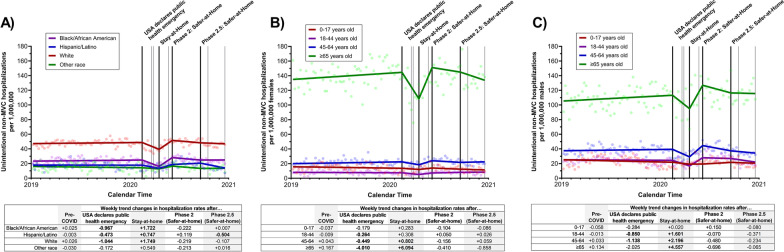
Results: There were 70,478 trauma hospitalizations in North Carolina, 2019-2020. In 2020, median age was 53 years old and 59% were male. Assault hospitalization rates (per 1,000,000 NC residents) increased after the Stay-at-Home order, but substantial increases were only observed among Black/African American residents (weekly trend change = 1.147, 95% CI = 0.634 to 1.662) and 18-44-year-old males (weekly trend change = 1.708, 95% CI = 0.870 to 2.545). After major restrictions were lifted, assault rates decreased but remained elevated compared to pre-COVID levels. Unintentional non-MVC injury hospitalizations decreased after the USA declared a public health emergency, especially among women ≥ 65 years old (weekly trend change = -4.010, 95% CI = -6.166 to -1.855), but returned to pre-pandemic levels within several months.
Conclusions: Statewide Stay-at-Home orders placed Black/African American residents at higher risk of assault hospitalizations, exacerbating pre-existing disparities. Males 18-44 years old were also at higher risk of assault hospitalization. Fear of COVID-19 may have led to decreases in unintentional non-MVC hospitalization rates, particularly among older females. Policy makers must anticipate policy-related harms that may disproportionately affect already disadvantaged communities and develop mitigation approaches.
Keywords: Assault; Motor vehicle collisions; Stay-at-Home; Trauma disparities.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures

Update of
-
Effect of Stay-at-Home Orders and Other COVID-Related Policies on Trauma Hospitalization Rates and Disparities in the United States: A Statewide Time-Series Analysis.medRxiv [Preprint]. 2022 Jul 12:2022.07.11.22277511. doi: 10.1101/2022.07.11.22277511. medRxiv. 2022. Update in: Inj Epidemiol. 2022 Nov 21;9(1):33. doi: 10.1186/s40621-022-00409-2. PMID: 35898348 Free PMC article. Updated. Preprint.
References
-
- Chiba H, Lewis M, Benjamin ER, Jakob DA, Liasidis P, Wong MD, et al. "Safer at home": the effect of the COVID-19 lockdown on epidemiology, resource utilization, and outcomes at a large urban trauma center. J Trauma Acute Care Surg. 2021;90(4):708–713. doi: 10.1097/TA.0000000000003061. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
