

Atypical enteropathogenic E. coli are associated with disease activity in ulcerative colitis
- PMID: 36415023
- PMCID: PMC9704410
- DOI: 10.1080/19490976.2022.2143218
Atypical enteropathogenic E. coli are associated with disease activity in ulcerative colitis
Abstract
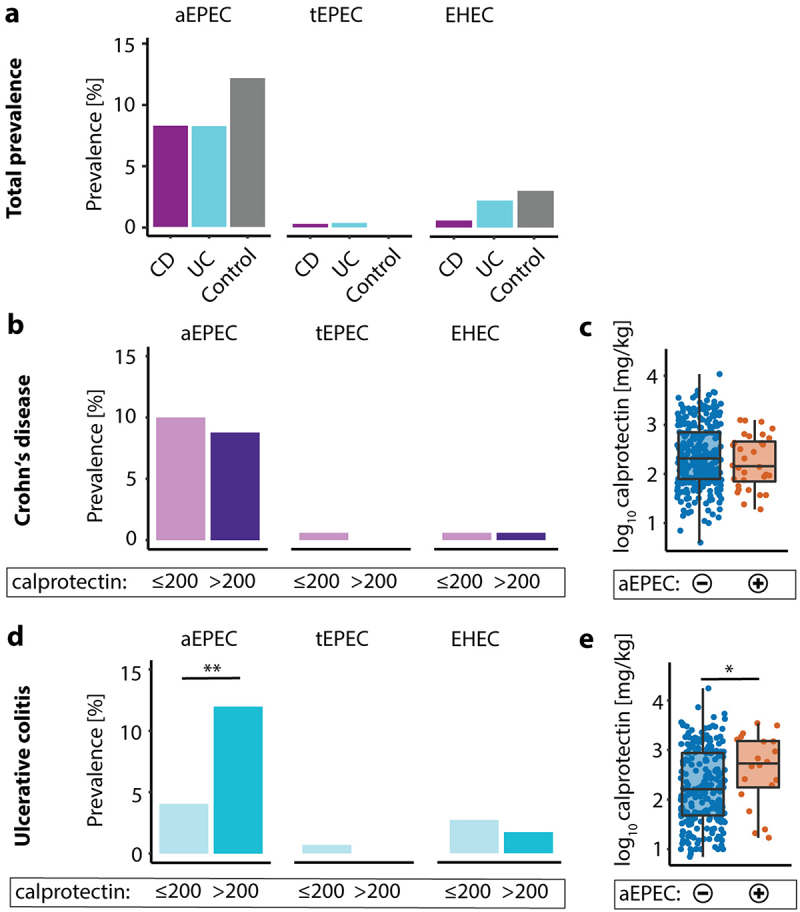
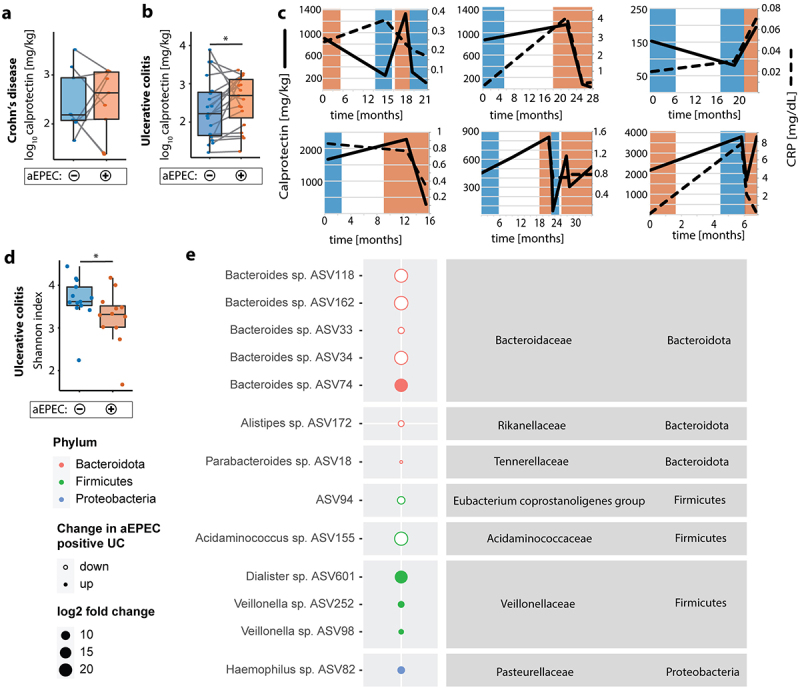
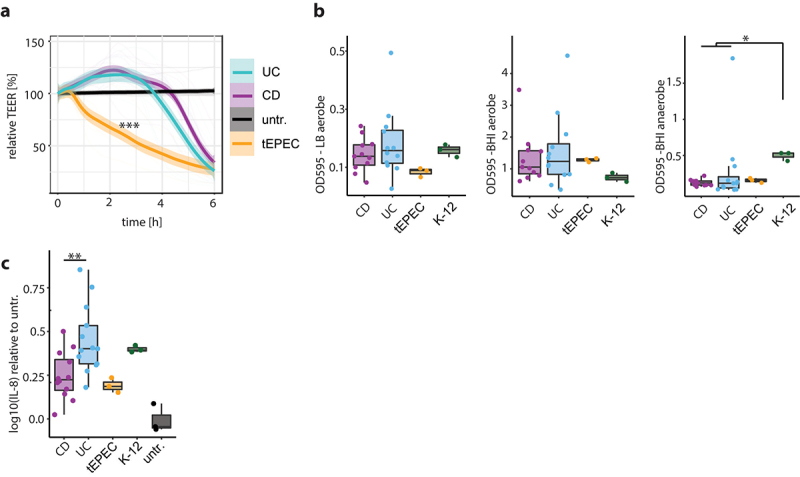
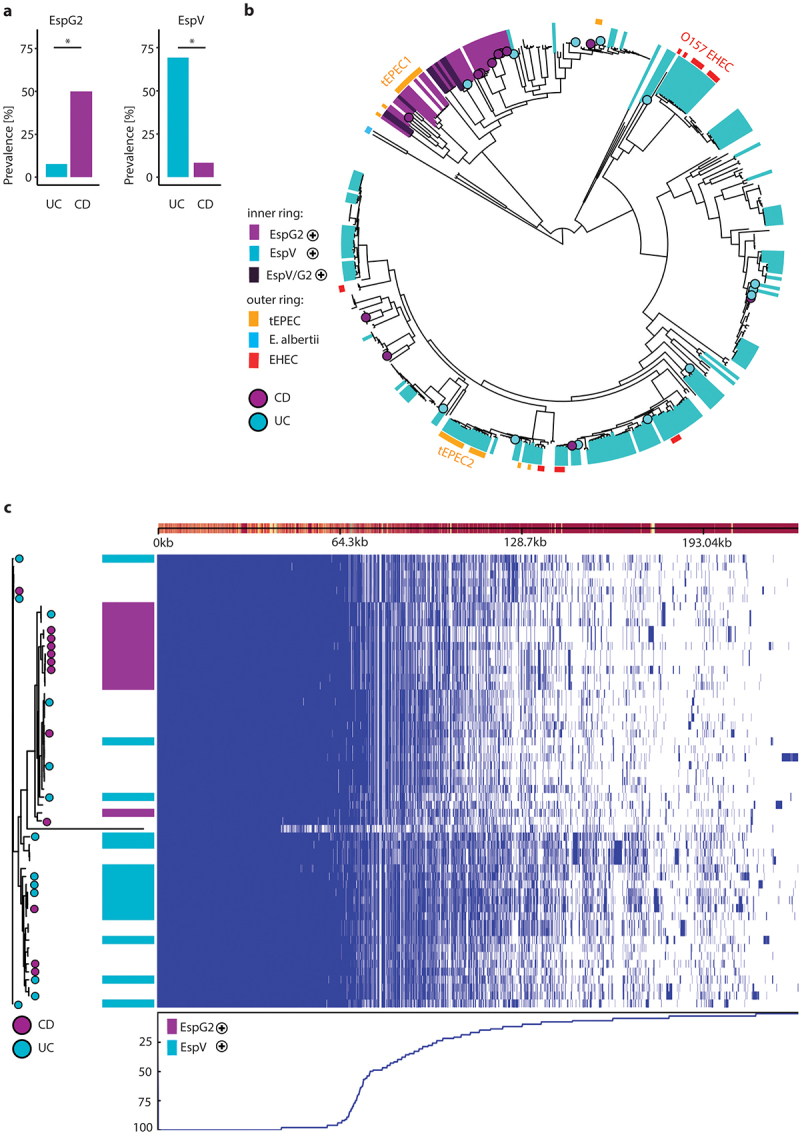
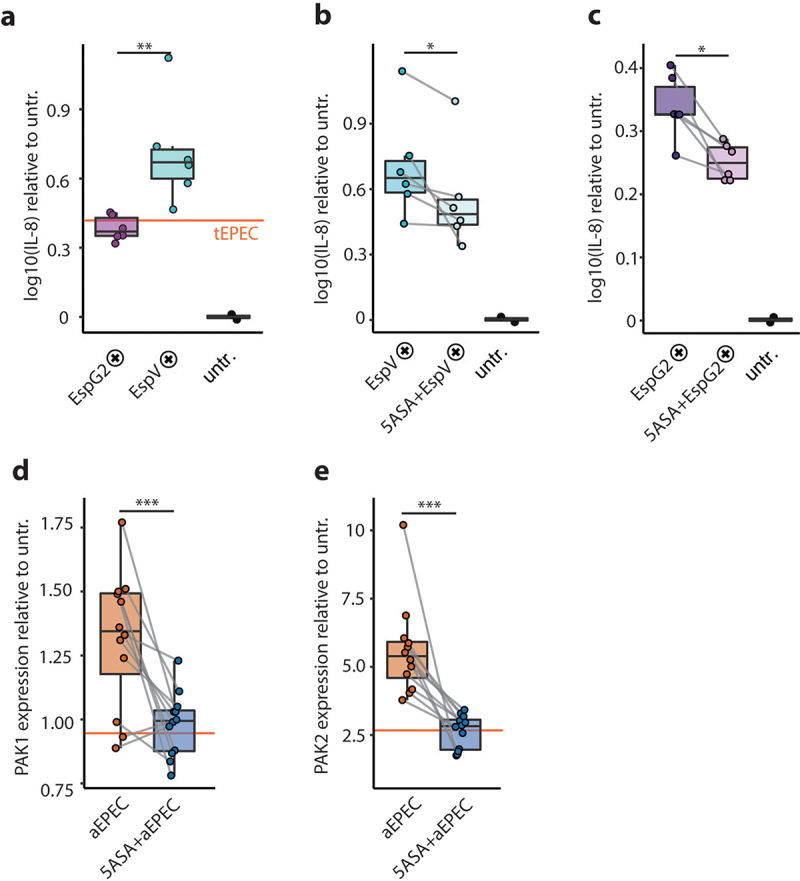
With increasing urbanization and industrialization, the prevalence of inflammatory bowel diseases (IBDs) has steadily been rising over the past two decades. IBD involves flares of gastrointestinal (GI) inflammation accompanied by microbiota perturbations. However, microbial mechanisms that trigger such flares remain elusive. Here, we analyzed the association of the emerging pathogen atypical enteropathogenic E. coli (aEPEC) with IBD disease activity. The presence of diarrheagenic E. coli was assessed in stool samples from 630 IBD patients and 234 age- and sex-matched controls without GI symptoms. Microbiota was analyzed with 16S ribosomal RNA gene amplicon sequencing, and 57 clinical aEPEC isolates were subjected to whole-genome sequencing and in vitro pathogenicity experiments including biofilm formation, epithelial barrier function and the ability to induce pro-inflammatory signaling. The presence of aEPEC correlated with laboratory, clinical and endoscopic disease activity in ulcerative colitis (UC), as well as microbiota dysbiosis. In vitro, aEPEC strains induce epithelial p21-activated kinases, disrupt the epithelial barrier and display potent biofilm formation. The effector proteins espV and espG2 distinguish aEPEC cultured from UC and Crohn's disease patients, respectively. EspV-positive aEPEC harbor more virulence factors and have a higher pro-inflammatory potential, which is counteracted by 5-ASA. aEPEC may tip a fragile immune-microbiota homeostasis and thereby contribute to flares in UC. aEPEC isolates from UC patients display properties to disrupt the epithelial barrier and to induce pro-inflammatory signaling in vitro.
Keywords: 5-ASA; Crohn's disease (CD); Escherichia coli (E. coli); Ulcerative colitis (UC); bacterial–epithelial interaction; effector proteins; enteropathogenic E. coli (EPEC); inflammatory bowel disease (IBD); microbiome; p21-activated kinase (PAK); virulence factors.
Conflict of interest statement
There is no competing interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous