

Retrospective Efficacy and Cost-Containment Assessment of 10 kHz Spinal Cord Stimulation (SCS) in Non-Surgical Refractory Back Pain Patients
- PMID: 36415659
- PMCID: PMC9676005
- DOI: 10.2147/JPR.S373873
Retrospective Efficacy and Cost-Containment Assessment of 10 kHz Spinal Cord Stimulation (SCS) in Non-Surgical Refractory Back Pain Patients
Abstract
Background: Non-surgical refractory back pain (NSRBP) is persistent, severe back pain that is not considered surgically correctable. Published studies have demonstrated clinically important long-term improvement in pain and functional capacity when 10kHz spinal cord stimulation (SCS) is used to treat NSRBP. This study examines if real-world patients in interventional pain practice obtain the same outcomes, and have any reduction in health care utilization (HCU) following 10kHz SCS implant.
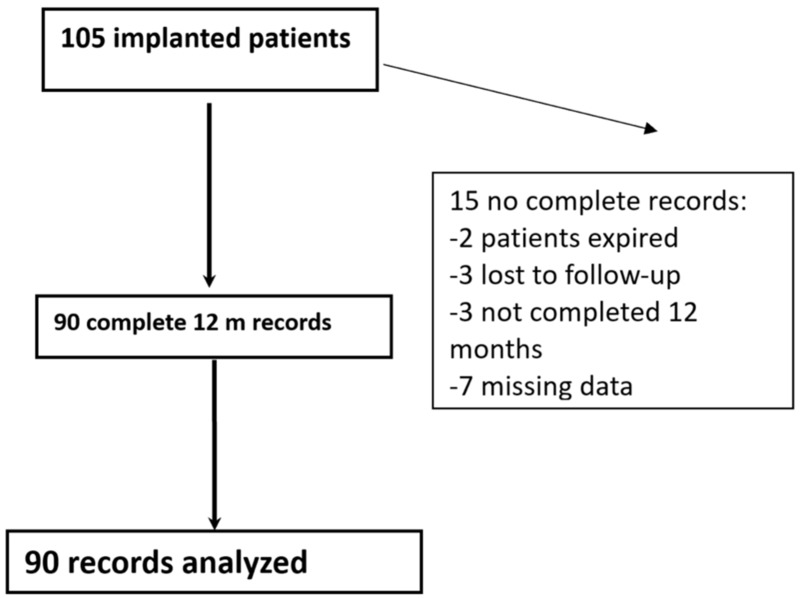
Methods: We conducted a retrospective chart review of 105 patients from two clinical sites who underwent implantation of 10kHz SCS for NSRBP. The three most frequent diagnoses were lumbosacral radiculopathy, degenerative disc disease (DDD)/discogenic back pain and foraminal stenosis. The complete set of patient-level electronic data, including clinical outcomes, HCU, and at least 12 months (12M) follow-up were available in 90 subjects.
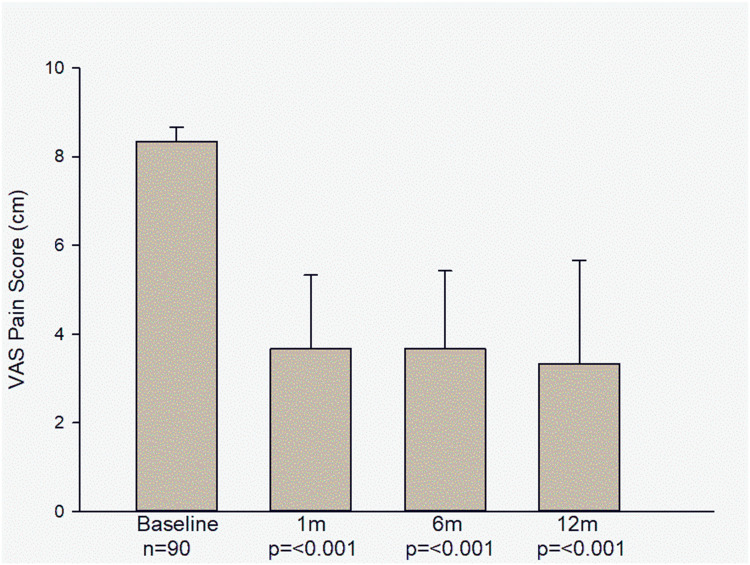
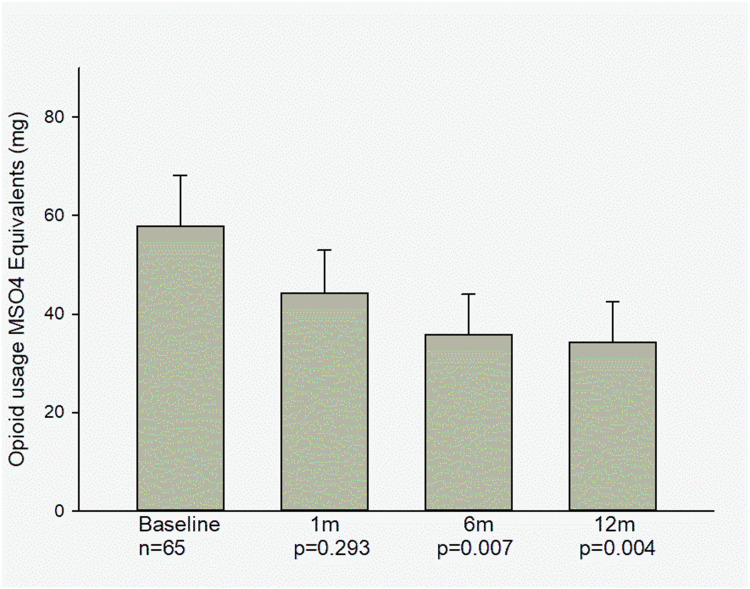
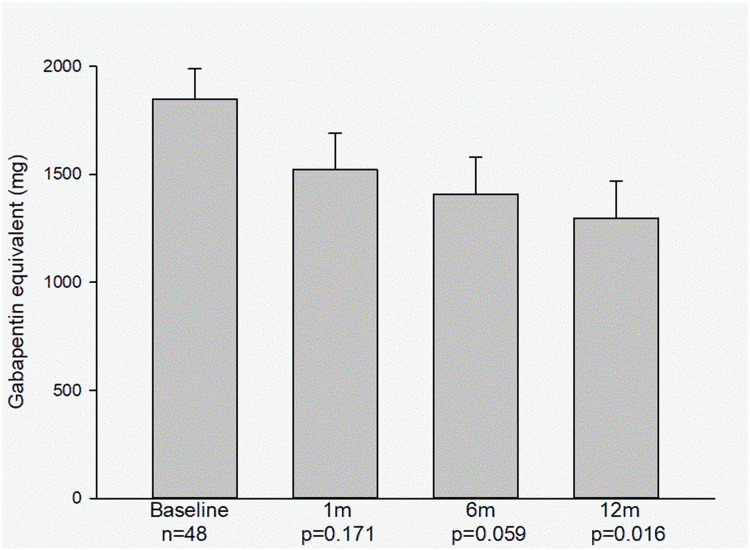
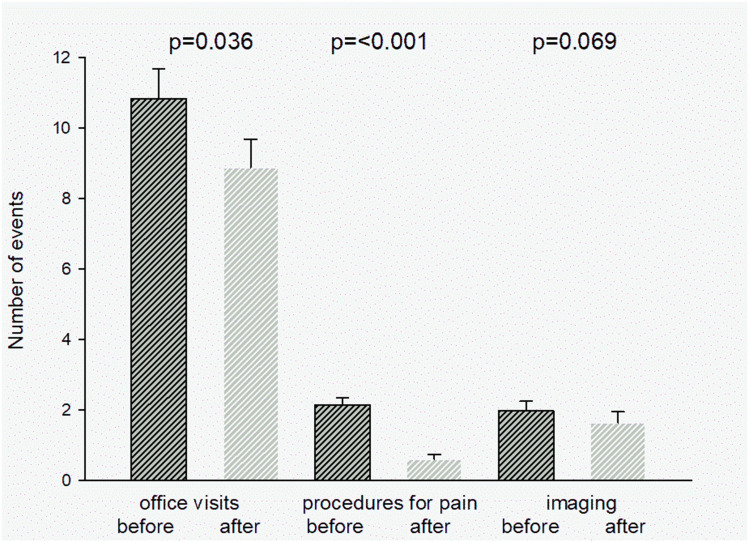
Results: The 90 analyzed patients were 63.9 years old (median 67) with an average of 10.2 years since back pain diagnosis. Reported pain on the Visual Analog Scale (VAS) decreased from 7.78±1.3 cm to 3.4±2.4 cm at 12M after SCS implant (p<0.001). Opioid usage (n = 65) decreased from 57.9±89.9 mg to 34.3±66.4 mg MSO4 equivalents (p = 0.004) at 12M. There were 46 patients on various doses of anticonvulsants, mostly gabapentin. The average dose decreased from 1847.91±973.6 mg at baseline to 1297.9±1184.6 mg at 12M after implant (p = 0.016). HCU was analyzed comparing the 12M before to the 12M after implant. Number of office visits decreased from 10.83±8.0 per year to 8.86±7.64 (p = 0.036), number of procedures to control chronic pain decreased from 2.2±1.9 to 0.6±1.2 (p<0.001). There was no significant change in number of imaging procedures, hospital admissions, or days spent in the hospital.
Conclusion: 10kHz SCS warrants consideration as a therapeutic option for NSRBP patients and appears to provide a substantial reduction in HCU in the year following implant.
Keywords: NSRBP; SCS; discogenic back pain; high-frequency 10 kHz spinal cord stimulation; lower back pain; lumbosacral radiculopathy; neuromodulation; non-surgical refractory back pain; spinal cord stimulation.
© 2022 Kapural and Calodney.
Conflict of interest statement
Drs Kapural and Calodney are paid consultants for Nevro Corp. Dr Leonardo Kapural also reports grants and/or personal fees from Medtronic, Biotronik, Nalu Medical, Saluda, and Gimer Medical, during the conduct of the study. Dr Aaron Calodney is consultant for Medtronic, Boston Scientific, Nevro, PainTeq, Stimwave, Stryker, and Vertos, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- Kapural L, Yu C, Doust MW, et al. Novel 10-kHz high-frequency therapy (HF10 therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZARCT randomized controlled trial. Anesthesiology. 2015;123:851–860. doi:10.1097/ALN.0000000000000774 - DOI - PubMed
-
- Kapural L, Yu C, Doust MW, et al. Comparison of 10-kHz highfrequency and traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: 24-month results from a multicenter, randomized, controlled pivotal trial. Neurosurgery. 2016;79:667. doi:10.1227/NEU.0000000000001418 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
