

Pharmacologic restraint use for children experiencing mental health crises in pediatric hospitals
- PMID: 36415909
- PMCID: PMC9899307
- DOI: 10.1002/jhm.13009
Pharmacologic restraint use for children experiencing mental health crises in pediatric hospitals
Abstract
Background: Children in mental health crises are increasingly admitted to children's hospitals awaiting inpatient psychiatric placement. During hospitalization, patients may exhibit acute agitation prompting pharmacologic restraint use.
Objective: To determine hospital-level incidence and variation of pharmacologic restraint use among children admitted for mental health conditions in children's hospitals.
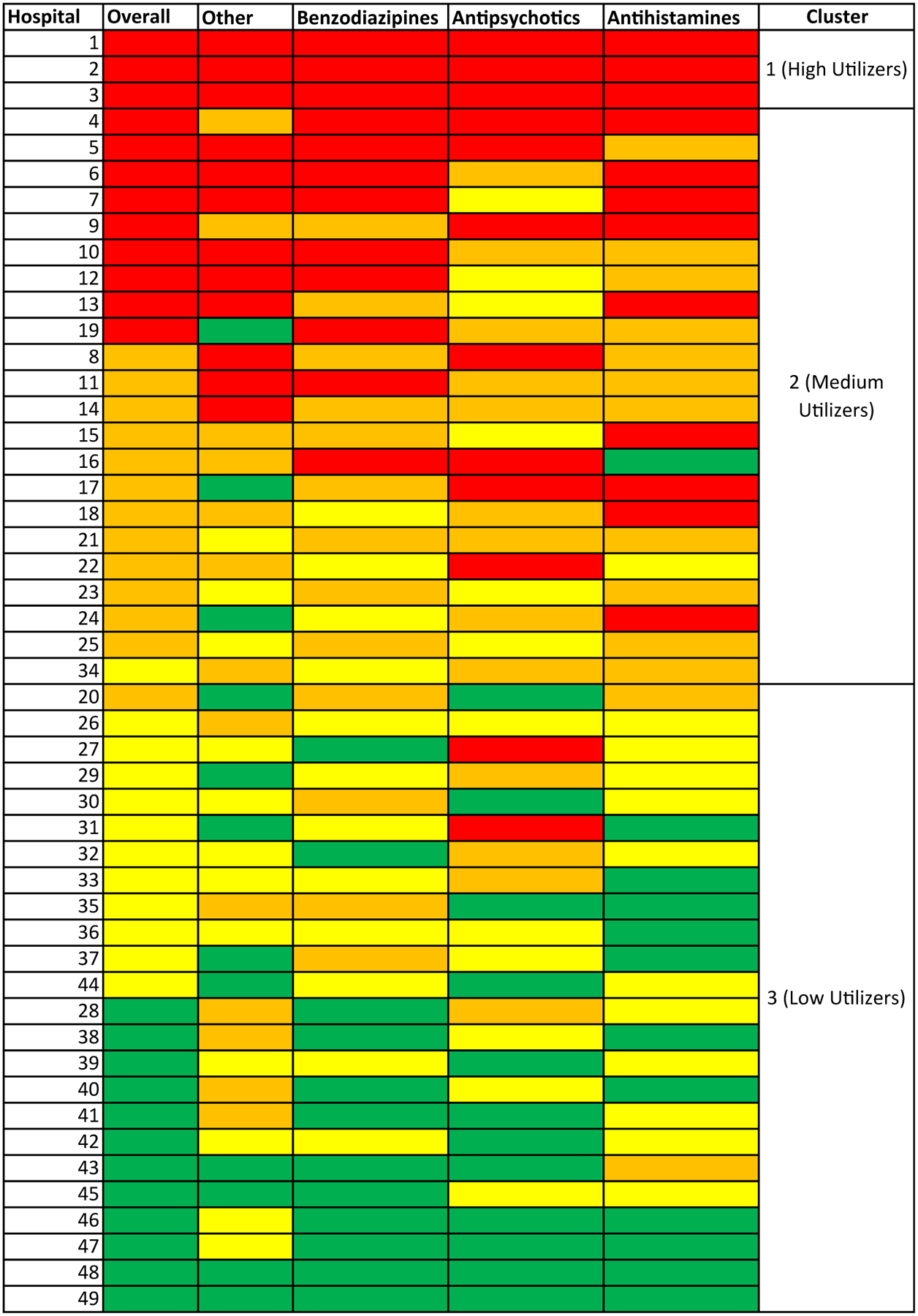
Design, setting, and participants: We examined data for children (5 to ≤18 years) admitted to children's hospitals with a primary mental health condition from 2018 to 2020 using the Pediatric Health Information System database. Hospital rates of parenteral pharmacologic restraint use per 1000 mental health bed days were determined and compared after adjusting for patient-level and demographic factors. Cluster analysis (k-means) was used to group hospitals based on overall restraint use (rate quartiles) and drug class. Hospital-level factors for pharmacologic restraint use were compared.
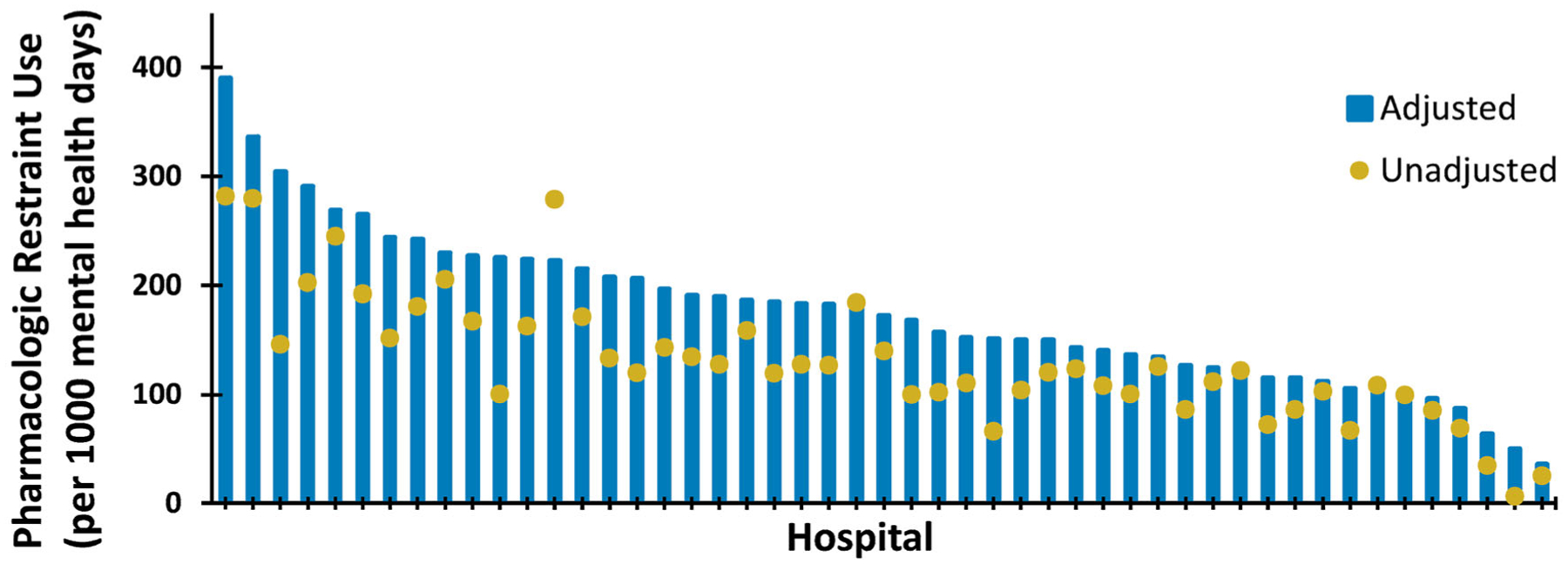
Results: Of 29,834 included encounters, 3747 (12.6%) had pharmacologic restraint use. Adjusted hospital rates ranged from 35 to 389 pharmacologic restraint use days per 1000 mental health bed days with a mean of 175 (standard deviation: 72). Cluster analysis revealed three hospitals were high utilizers of all drug classes. No significant differences in pharmacologic restraint use were found in the hospital-level analysis.
Conclusions: Children's hospitals demonstrate wide variation in pharmacologic restraint rates for mental health hospitalizations, with a 10-fold difference in adjusted rates between highest and lowest utilizers, and high overall utilizers order medications across all drug classes.
© 2022 Society of Hospital Medicine.
Conflict of interest statement
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Figures
Comment in
-
Rethinking restraint use during pediatric mental health hospitalizations.J Hosp Med. 2023 Feb;18(2):196-197. doi: 10.1002/jhm.13015. Epub 2022 Nov 27. J Hosp Med. 2023. PMID: 36437537 No abstract available.
Similar articles
-
Disparities in Pharmacologic Restraint for Children Hospitalized in Mental Health Crisis.Pediatrics. 2024 Jan 1;153(1):e2023061353. doi: 10.1542/peds.2023-061353. Pediatrics. 2024. PMID: 38073320 Free PMC article.
-
Pharmacologic Restraint Use During Mental Health Admissions to Children's Hospitals.Pediatrics. 2024 Jan 1;153(1):e2023062784. doi: 10.1542/peds.2023-062784. Pediatrics. 2024. PMID: 38073316
-
Patient Risk Factors for Violent Restraint Use in a Children's Hospital Medical Unit.Hosp Pediatr. 2021 Aug;11(8):833-840. doi: 10.1542/hpeds.2020-000273. Epub 2021 Jul 6. Hosp Pediatr. 2021. PMID: 34230060 Free PMC article.
-
Pharmacologic Restraint Use During Mental Health Visits in Pediatric Emergency Departments.J Pediatr. 2021 Sep;236:276-283.e2. doi: 10.1016/j.jpeds.2021.03.027. Epub 2021 Mar 24. J Pediatr. 2021. PMID: 33771581
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
Cited by
-
Disparities in Pharmacologic Restraint for Children Hospitalized in Mental Health Crisis.Pediatrics. 2024 Jan 1;153(1):e2023061353. doi: 10.1542/peds.2023-061353. Pediatrics. 2024. PMID: 38073320 Free PMC article.
-
Pediatric Physical Restraint Coding in US Hospitals: A 2019 Kids Inpatient Database Study.Hosp Pediatr. 2024 May 1;14(5):337-347. doi: 10.1542/hpeds.2023-007562. Hosp Pediatr. 2024. PMID: 38567417 Free PMC article.
References
-
- American Academy of Pediatrics. AAP-AACAP-CHA Declaration of a National Emergency in Child and Adolescent Mental Health. American Academy of Pediatrics; 2022. http://www.aap.org/en/advocacy/child-and-adolescent-healthy-mental-devel...
-
- Chun TH, Katz ER, Duffy SJ, Gerson RS. Challenges of managing pediatric mental health crises in the emergency department. Child Adolesc Psychiatr Clin N Am. 2015;24(1):21–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
