

Myelofibrosis
- PMID: 36416738
- PMCID: PMC10646775
- DOI: 10.1182/blood.2022017423
Myelofibrosis
Abstract
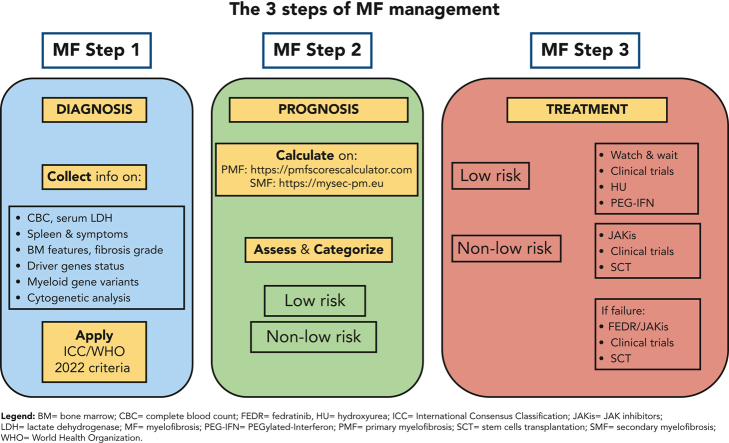
The clinical phenotype of primary and post-polycythemia vera and postessential thrombocythemia myelofibrosis (MF) is dominated by splenomegaly, symptomatology, a variety of blood cell alterations, and a tendency to develop vascular complications and blast phase. Diagnosis requires assessing complete cell blood counts, bone marrow morphology, deep genetic evaluations, and disease history. Driver molecular events consist of JAK2V617F, CALR, and MPL mutations, whereas about 8% to 10% of MF are "triple-negative." Additional myeloid-gene variants are described in roughly 80% of patients. Currently available clinical-based and integrated clinical/molecular-based scoring systems predict the survival of patients with MF and are applied for conventional treatment decision-making, indication to stem cell transplant (SCT) and allocation in clinical trials. Standard treatment consists of anemia-oriented therapies, hydroxyurea, and JAK inhibitors such as ruxolitinib, fedratinib, and pacritinib. Overall, spleen volume reduction of 35% or greater at week 24 can be achieved by 42% of ruxolitinib-, 47% of fedratinib-, 19% of pacritinib-, and 27% of momelotinib-treated patients. Now, it is time to move towards new paradigms for evaluating efficacy like disease modification, that we intend as a robust and unequivocal effect on disease biology and/or on patient survival. The growing number of clinical trials potentially pave the way for new strategies in patients with MF. Translational studies of some molecules showed an early effect on bone marrow fibrosis and on variant allele frequencies of myeloid genes. SCT is still the only curative option, however, it is associated with relevant challenges. This review focuses on the diagnosis, prognostication, and treatment of MF.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: F.P. received honoraria for lectures and advisory boards from Novartis, Bristol-Myers Squibb/Celgene, Sierra Oncology, AbbVie, Janssen, Roche, AOP Orphan, Karyopharm, Kyowa Kirin, and MEI. B.M. received honoraria for lectures from Novartis.
Figures

Comment in
-
Introduction to a review series on classic myeloproliferative neoplasms.Blood. 2023 Apr 20;141(16):1897-1899. doi: 10.1182/blood.2023019876. Blood. 2023. PMID: 36867843 No abstract available.
References
-
- Cervantes F, Dupriez B, Pereira A, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for myelofibrosis research and treatment. Blood. 2009;113(13):2895–2901. - PubMed
-
- Vainchenker W, Kralovics R. Genetic basis and molecular pathophysiology of classical myeloproliferative neoplasms. Blood. 2017;129(6):667–679. - PubMed
-
- Passamonti F, Mora B, Giorgino T, et al. Driver mutations’ effect in secondary myelofibrosis: an international multicenter study based on 781 patients. Leukemia. 2017;31(4):970–973. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
