

CD19/CD20 Bispecific Chimeric Antigen Receptor (CAR) in Naive/Memory T Cells for the Treatment of Relapsed or Refractory Non-Hodgkin Lymphoma
- PMID: 36416874
- PMCID: PMC9992104
- DOI: 10.1158/2159-8290.CD-22-0964
CD19/CD20 Bispecific Chimeric Antigen Receptor (CAR) in Naive/Memory T Cells for the Treatment of Relapsed or Refractory Non-Hodgkin Lymphoma
Abstract
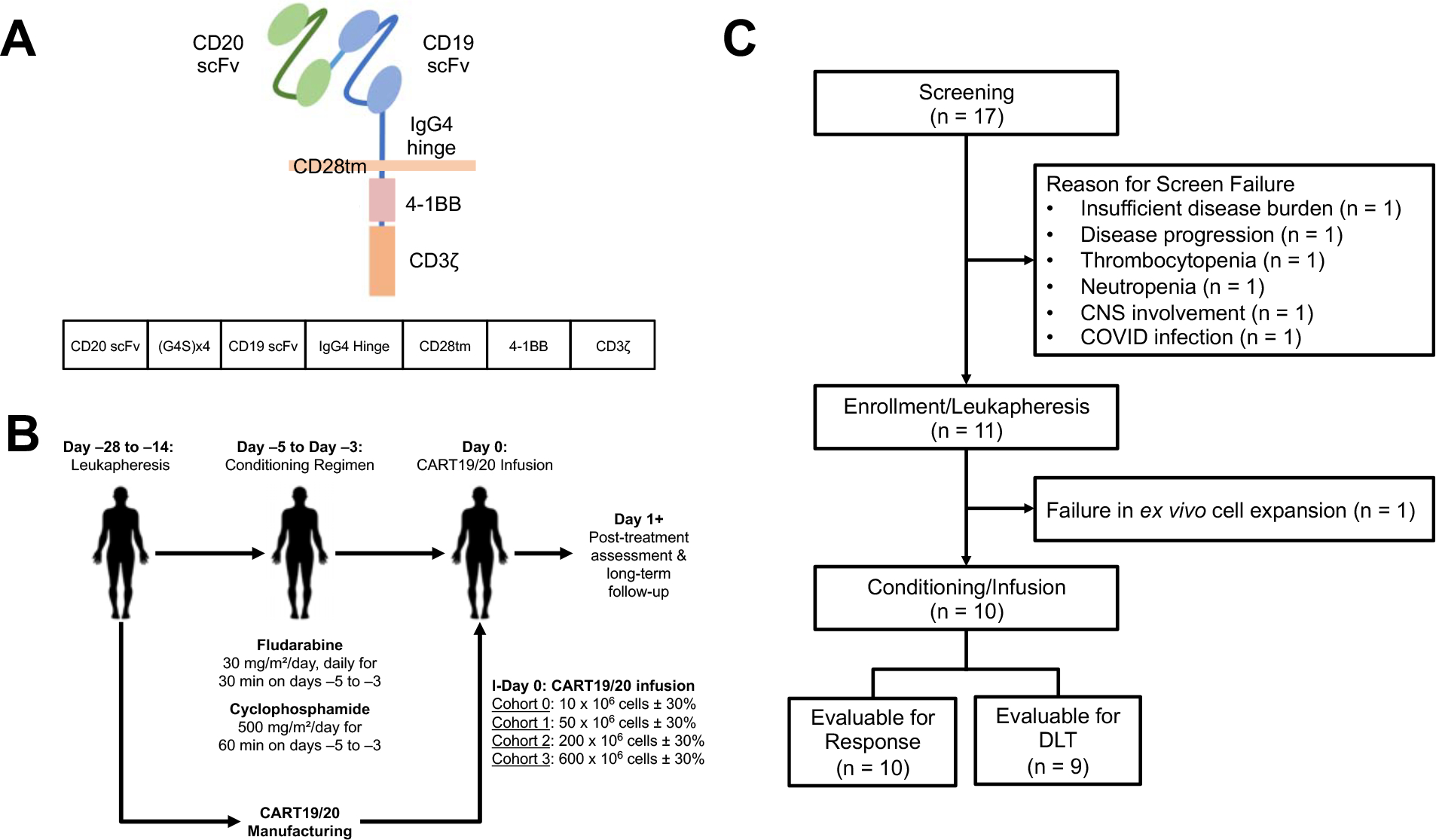
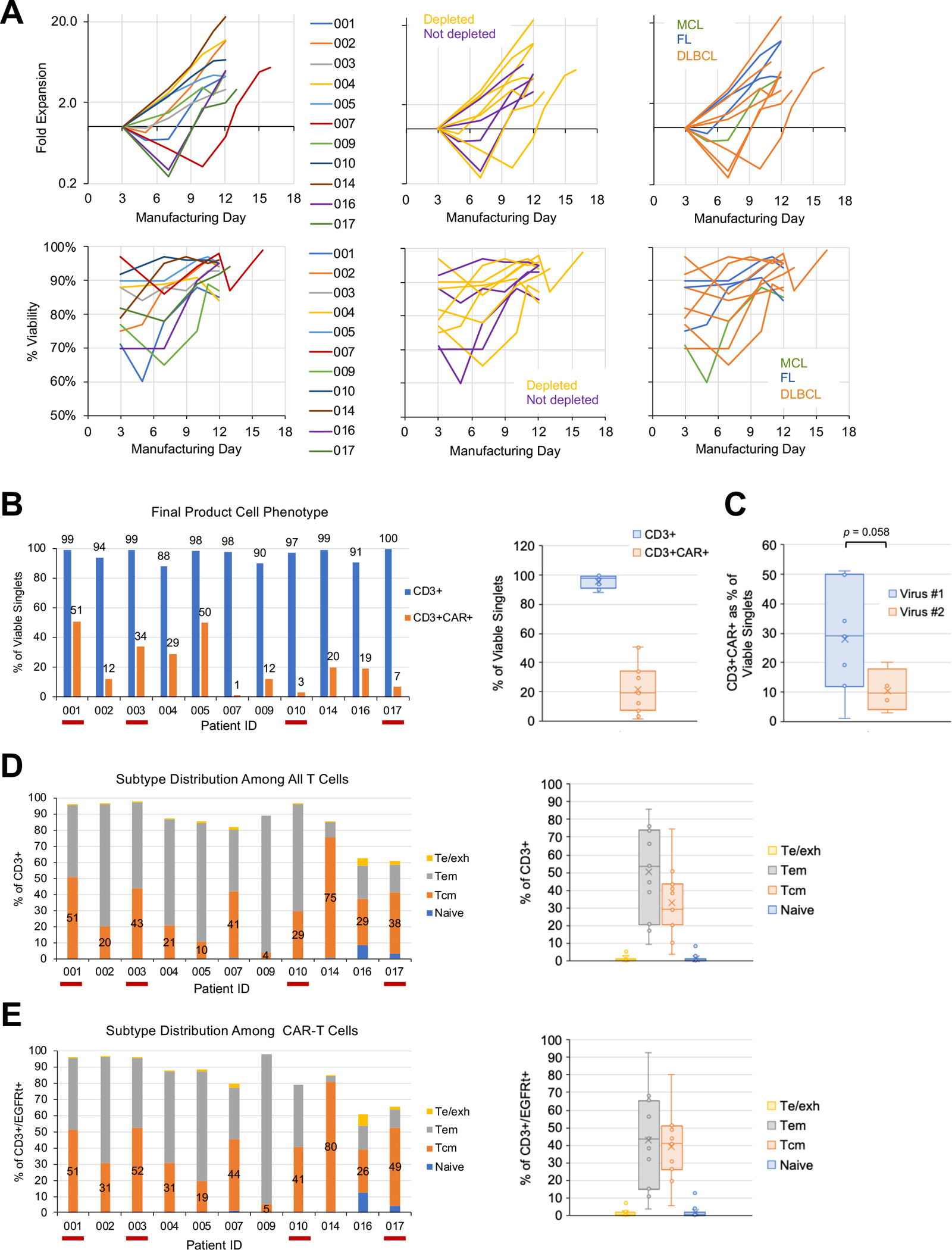
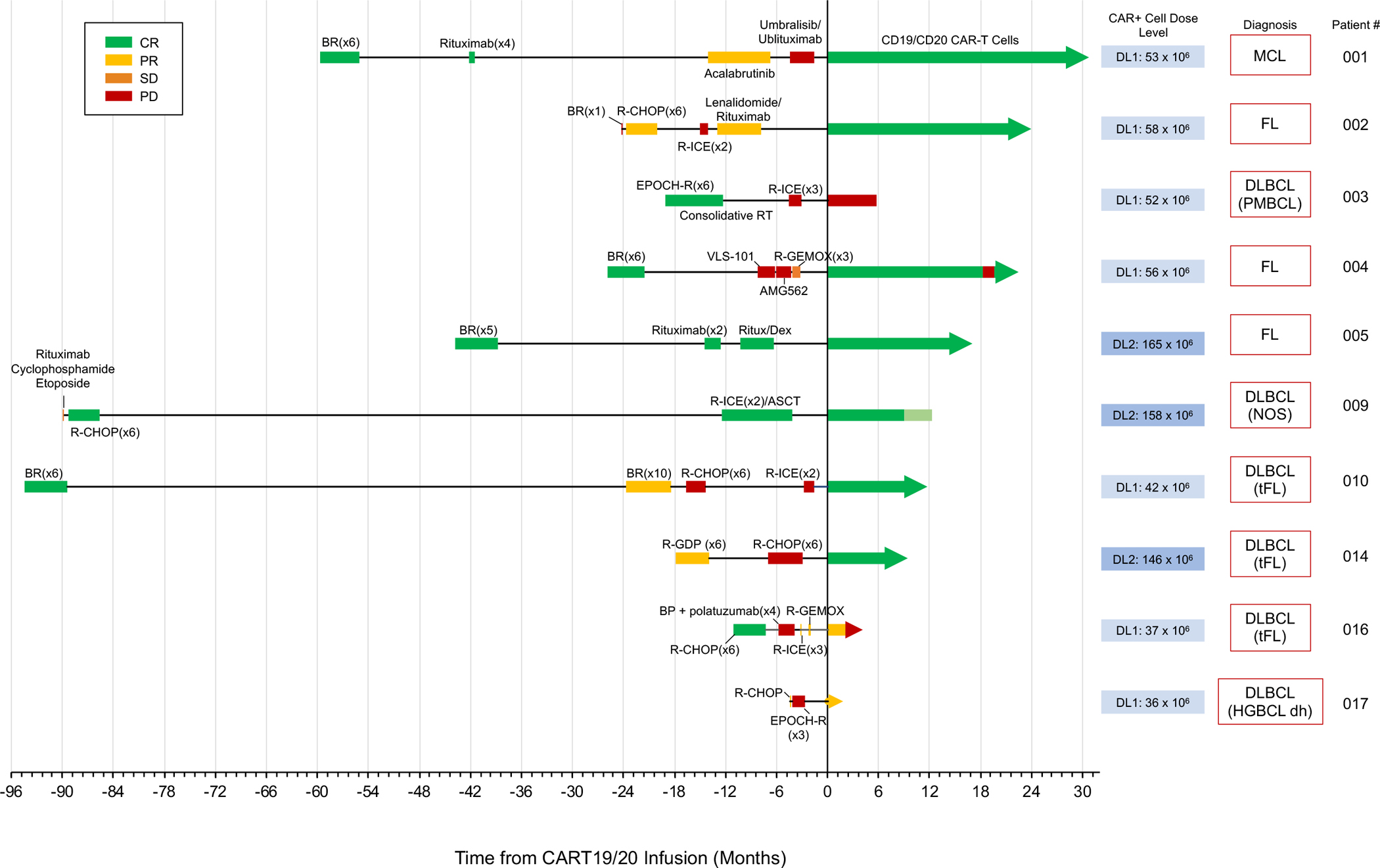
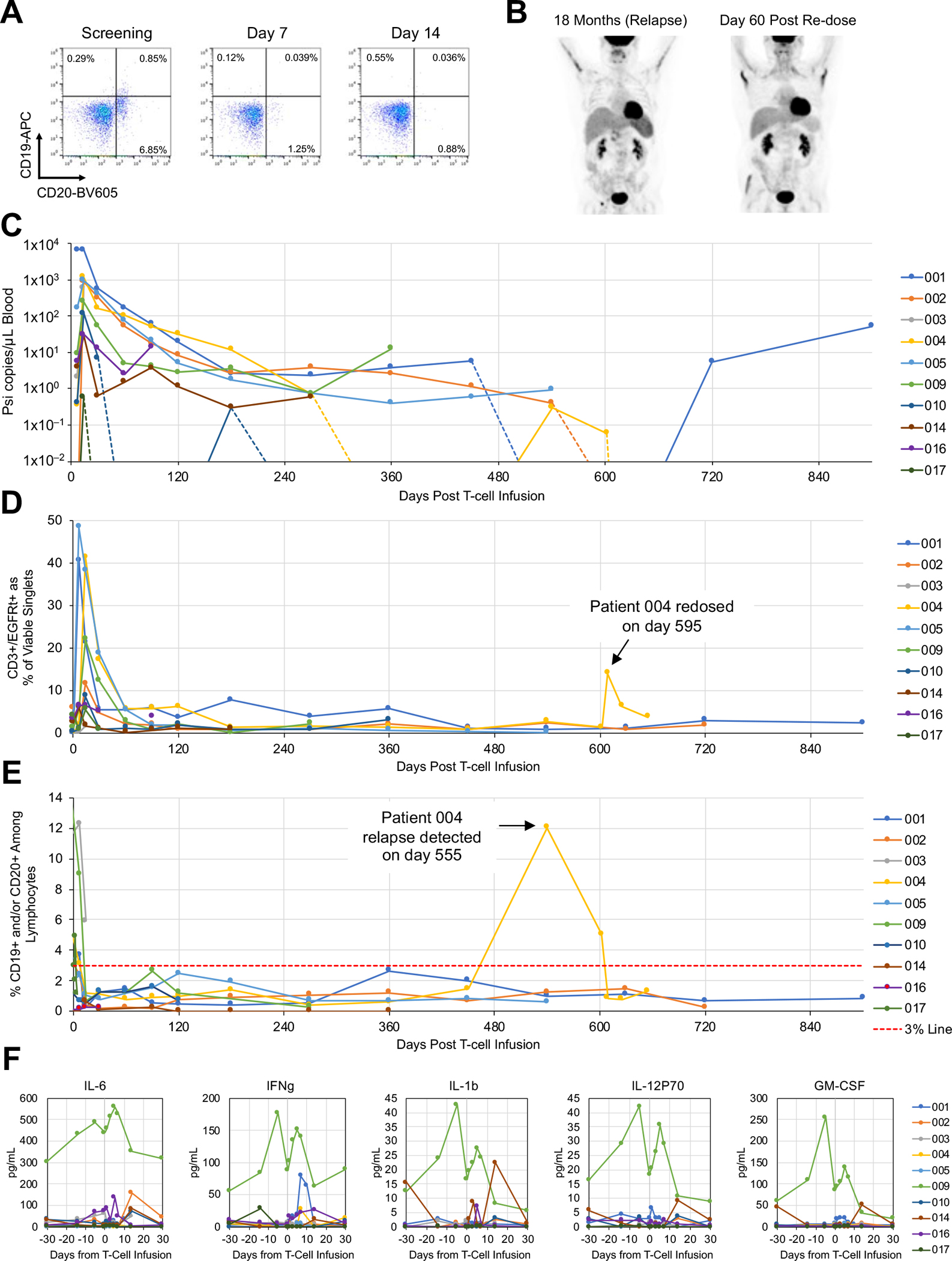
To address antigen escape and loss of T-cell functionality, we report a phase I clinical trial (NCT04007029) evaluating autologous naive and memory T (TN/MEM) cells engineered to express a bispecific anti-CD19/CD20 chimeric antigen receptor (CAR; CART19/20) for patients with relapsed/refractory non-Hodgkin lymphoma (NHL), with safety as the primary endpoint. Ten patients were treated with 36 × 106 to 165 × 106 CART19/20 cells. No patient experienced neurotoxicity of any grade or over grade 1 cytokine release syndrome. One case of dose-limiting toxicity (persistent cytopenia) was observed. Nine of 10 patients achieved objective response [90% overall response rate (ORR)], with seven achieving complete remission [70% complete responses (CR) rate]. One patient relapsed after 18 months in CR but returned to CR after receiving a second dose of CART19/20 cells. Median progression-free survival was 18 months and median overall survival was not reached with a 17-month median follow-up. In conclusion, CART19/20 TN/MEM cells are safe and effective in patients with relapsed/refractory NHL, with durable responses achieved at low dosage levels.
Significance: Autologous CD19/CD20 bispecific CAR-T cell therapy generated from TN/MEM cells for patients with NHL is safe (no neurotoxicity, maximum grade 1 cytokine release syndrome) and demonstrates strong efficacy (90% ORR, 70% CR rate) in a first-in-human, phase I dose-escalation trial. This article is highlighted in the In This Issue feature, p. 517.
©2022 American Association for Cancer Research.
Conflict of interest statement
COMPETING INTERESTS
Y.Y.C. is an inventor on a patent application for CART19/20 and holds several patent applications in the area of CAR-T cell therapy. Y.Y.C. is a founder of, holds equity in, and receives consulting fees from ImmPACT Bio. She is a member of the scientific advisory board of and holds equity in Catamaran Bio, Notch Therapeutics, Pluto Immunotherapeutics, Prime Medicine, Sonoma Biotherapeutics, and Waypoint Bio. She has consulted for Novartis and Gritstone Bio. S.M.L. holds equity in 1200 Pharma and TORL BioTherapeutics, and has received research funding from Abbvie, Bioline, Bristol Myers Squibb (BMS), Janssen, Novartis, Pfizer, and Sanofi. C.M.W. is a current employee of and holds equity in Orca Bio. J.T. is a current employee of and holds equity in ImmPACT Bio. M.R. is a current employee of and holds equity in Fate Therapeutics. G.J.S. holds equity in Amgen, BMS, and Johnson & Johnson; has consulted for or received honoraria from Kite, Astellas, AbbVie, Incyte, BMS, Stemline, Karyopharm, Agios, Amgen, AstraZenecca, Novartis, Ono Pharma, Celgene, and Jazz; and has received research funding from Actinium, Actuate, AbbVie, AltruBio, Arog, Astellas, AVM Biopharma, Cellectis, Celgene, Cellerant, Constellation, CTI, Forma, Cyclacel, Daiichi-Sankyo, Deciphera, Ifly, FujiFilm, Gamida, Gilead, Genetech/Roche, Geron, Glycomimetics, Incyte, Janssen, Karyopharm, Kite, Mateon, Medimmune, Millenium, Novartis, Onconova, Pfizer, PreCOG, Regimmune, Samus, Sellas, Sangamo, Semline, Takeda, Tolero, and Trovagene. A.R. has received honoraria from consulting with Cstone, Merck, and Vedanta, is or has been a member of the scientific advisory board and holds stock in Advaxis, Appia, Apricity, Arcus, Compugen, CytomX, Highlight, ImaginAb, ImmPact, ImmuneSensor, Inspirna, Isoplexis, Kite-Gilead, Lutris, MapKure, Merus, PACT, Pluto, RAPT, Synthekine and Tango, has received research funding from Agilent and from Bristol-Myers Squibb through Stand Up to Cancer (SU2C), and patent royalties from Arsenal Bio. The other authors declare no conflicts of interest.
Figures

References
-
- Lee DW, Kochenderfer JN, Stetler-Stevenson M, Cui YK, Delbrook C, Feldman SA, et al. T cells expressing CD19 chimeric antigen receptors for acute lymphoblastic leukaemia in children and young adults: a phase 1 dose-escalation trial. Lancet 2015;385(9967):517–28 doi 10.1016/S0140-6736(14)61403-3.. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
