

The neurocognitive disorder cohort RIFADE: Aims, methods, first results showing cognitive improvement in a subgroup
- PMID: 36416960
- PMCID: PMC10238319
- DOI: 10.1007/s00406-022-01516-3
The neurocognitive disorder cohort RIFADE: Aims, methods, first results showing cognitive improvement in a subgroup
Abstract
Background: The NCD cohort study RIFADE (RIsk FActors of DEmentia) investigates the interaction of risk factors and neurocognitive disorders (NCDs) due to Alzheimer's disease (NCD-AD) and NCD of vascular type (NCD-vascular). Retrospective recruitment referred to a period from 2007 to 2018 in a single centre. In addition to the baseline visit, follow-up visits took place at 3, 6, 12 months followed by yearly visits. Visit times varied in part depending on adherence. The study also comprises an EEG bank and a bank with cerebral MRI (c-MRI).
Methods: Inclusion criteria were broad in order to cover a wide range of patterns of NCD. At baseline, patients underwent a large panel of assessments, e.g. including clinical history, diagnostic evaluation for NCD according to DSM-IV and NINDS AIREN criteria, a cognitive test battery including the DemTect, the clock drawing test and the Instrumental-Activities-of-Daily-Living-scale of Lawton and Brodie, EEG and c-MRI. At each follow-up visit, cognitive tests were repeated, in most cases also EEGs and in some cases c-MRIs. Numerous risk factors (RF) including vascular RF, atrial fibrillation, heart failure, sleep apnoea and lifestyle factors such as sedentary lifestyle, low cognitive style and smoking were evaluated for presence and for correction status at each visit, and modulation of uncorrected RF was initiated.
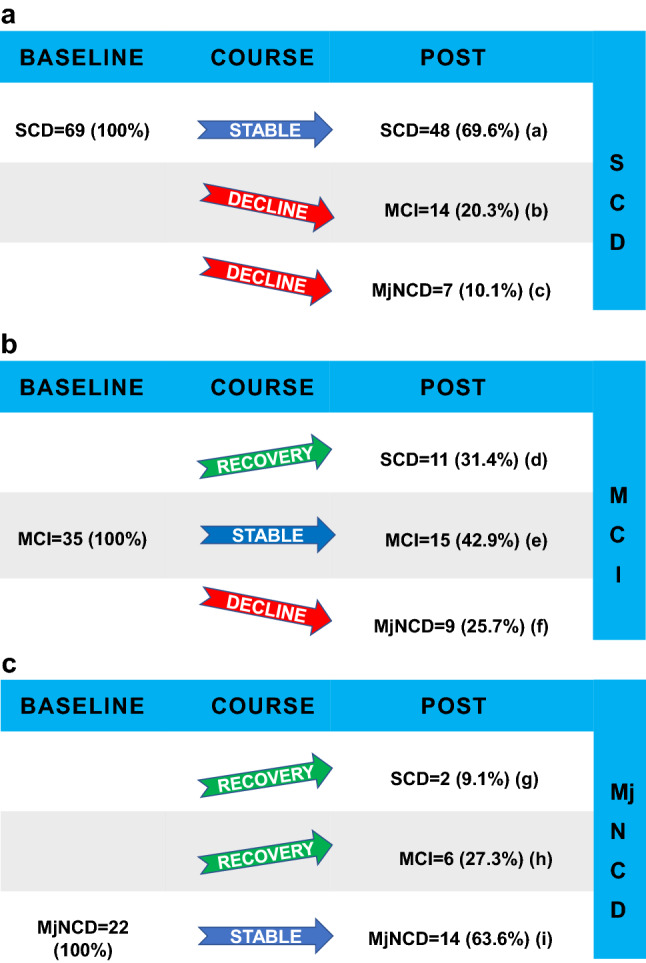
Results: Overall, 126 subjects with a clinical diagnosis of NCD were included (52% female, mean age 71 ± 10.6 years (range 35e86)), number of follow-up visits per subject 2.9 ± 2.4, observation time per subject 3.4 ± 2.8 years). Of these, 55/28/17% presented with the clinical stages subjective cognitive decline (SCD)/mild cognitive impairment (MCI)/dementia (major NCD). Clinical diagnoses, retrospectively re-evaluated according to DSM-5, were 5/21/68/6% Alzheimer´s disease (NCD-AD)/vascular NCD (NCD-vascular) / mixed NCD (NCD-AD + NCD-vascular)/unspecified NCD. First longitudinal results revealed a mean DemTect score at baseline 12.6 ± 4.2 vs last visit 12.0 ± 4.8 (p = 0.08) and a clock drawing test score at baseline 1.9 ± 1.3 vs last visit 2.3 ± 1.5 (p < 0.0001). Of all subjects with MCI or major NCD (n = 57), 19 improved in the clinical stage from baseline to last visit (33.3%). Sixteen subjects progressed from SCD or MCI (n = 104) to major NCD (15.4%).
Conclusion: The German NCD cohort RIFADE comprises patients with all clinical stages of NCD. A considerable subgroup improved in clinical stage. Further analysis is needed to answer the question of whether modulation of multiple risk factors provides a favourable effect on cognitive outcome in NCD.
Keywords: Dementia; Mild cognitive impairment; Neurocognitive disorder; Prevention and control; Risk factors.
© 2022. The Author(s).
Conflict of interest statement
The authors have not conflicts of interest to disclose in relation to the present article.
Figures

References
-
- World Health Organization (2021). Dementia. https://www.who.int/news-room/fact-sheets/detail/dementia
-
- von Siemens SM, Perneczky R, Vogelmeier CF, Behr J, Kauffmann-Guerrero D, Alter P, Kahnert K. The association of cognitive functioning as measured by the DemTect with functional and clinical characteristics of COPD: results from the COSYCONET cohort. Respir Res. 2019;20(1):1–13. doi: 10.1186/s12931-019-1217-5. - DOI - PMC - PubMed
-
- Bäckman L, MacDonald SW. Death and cognition: Viewing a 1962 concept through 2006 spectacles. Eur Psychol. 2006;11(3):161. doi: 10.1027/1016-9040.11.3.161. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
