

Measurement of airborne particle emission during surgical and percutaneous dilatational tracheostomy COVID-19 adapted procedures in a swine model: Experimental report and review of literature
- PMID: 36417482
- PMCID: PMC9683587
- DOI: 10.1371/journal.pone.0278089
Measurement of airborne particle emission during surgical and percutaneous dilatational tracheostomy COVID-19 adapted procedures in a swine model: Experimental report and review of literature
Abstract
Introduction: Surgical tracheostomy (ST) and Percutaneous dilatational tracheostomy (PDT) are classified as high-risk aerosol-generating procedures and might lead to healthcare workers (HCW) infection. Albeit the COVID-19 strain slightly released since the vaccination era, preventing HCW from infection remains a major economical and medical concern. To date, there is no study monitoring particle emissions during ST and PDT in a clinical setting. The aim of this study was to monitor particle emissions during ST and PDT in a swine model.
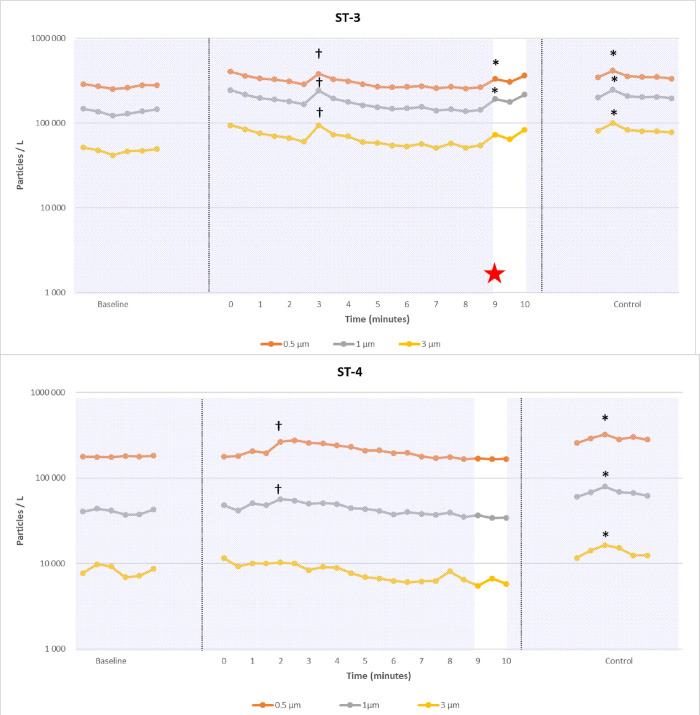
Methods: A randomized animal study on swine model with induced acute respiratory distress syndrome (ARDS) was conducted. A dedicated room with controlled airflow was used to standardize the measurements obtained using an airborne optical particle counter. 6 ST and 6 PDT were performed in 12 pigs. Airborne particles (diameter of 0.5 to 3 μm) were continuously measured; video and audio data were recorded. The emission of particles was considered as significant if the number of particles increased beyond the normal variations of baseline particle contamination determinations in the room. These significant emissions were interpreted in the light of video and audio recordings. Duration of procedures, number of expiratory pauses, technical errors and adverse events were also analyzed.
Results: 10 procedures (5 ST and 5 PDT) were fully analyzable. There was no systematic aerosolization during procedures. However, in 1/5 ST and 4/5 PDT, minor leaks and some adverse events (cuff perforation in 1 ST and 1 PDT) occurred. Human factors were responsible for 1 aerosolization during 1 PDT procedure. ST duration was significantly shorter than PDT (8.6 ± 1.3 vs 15.6 ± 1.9 minutes) and required less expiratory pauses (1 vs 6.8 ± 1.2).
Conclusions: COVID-19 adaptations allow preventing for major aerosol leaks for both ST and PDT, contributing to preserving healthcare workers during COVID-19 outbreak, but failed to achieve a perfectly airtight procedure. However, with COVID-19 adaptations, PDT required more expiratory pauses and more time than ST. Human factors and adverse events may lead to aerosolization and might be more frequent in PDT.
Copyright: © 2022 Favier et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
