

Rationale and design for the myocardial ischemia and transfusion (MINT) randomized clinical trial
- PMID: 36417955
- PMCID: PMC9928777
- DOI: 10.1016/j.ahj.2022.11.015
Rationale and design for the myocardial ischemia and transfusion (MINT) randomized clinical trial
Abstract
Background: Accumulating evidence from clinical trials suggests that a lower (restrictive) hemoglobin threshold (<8 g/dL) for red blood cell (RBC) transfusion, compared with a higher (liberal) threshold (≥10 g/dL) is safe. However, in anemic patients with acute myocardial infarction (MI), maintaining a higher hemoglobin level may increase oxygen delivery to vulnerable myocardium resulting in improved clinical outcomes. Conversely, RBC transfusion may result in increased blood viscosity, vascular inflammation, and reduction in available nitric oxide resulting in worse clinical outcomes. We hypothesize that a liberal transfusion strategy would improve clinical outcomes as compared to a more restrictive strategy.
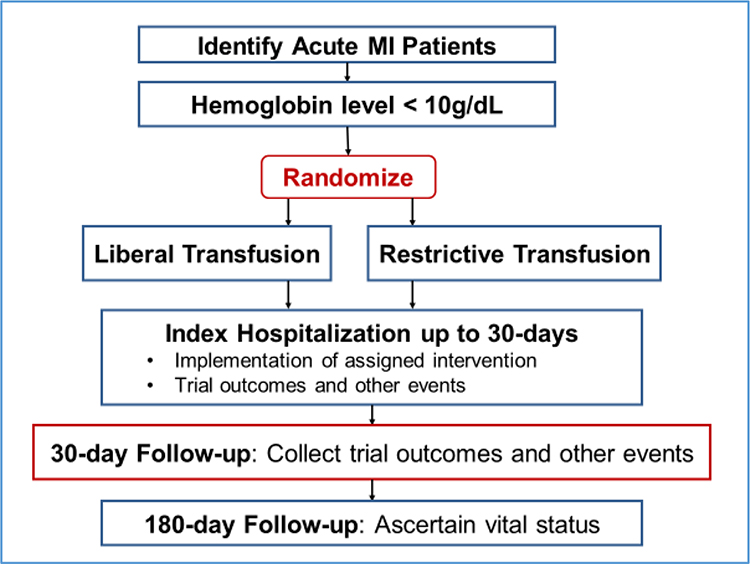
Methods: We will enroll 3500 patients with acute MI (type 1, 2, 4b or 4c) as defined by the Third Universal Definition of MI and a hemoglobin <10 g/dL at 144 centers in the United States, Canada, France, Brazil, New Zealand, and Australia. We randomly assign trial participants to a liberal or restrictive transfusion strategy. Participants assigned to the liberal strategy receive transfusion of RBCs sufficient to raise their hemoglobin to at least 10 g/dL. Participants assigned to the restrictive strategy are permitted to receive transfusion of RBCs if the hemoglobin falls below 8 g/dL or for persistent angina despite medical therapy. We will contact each participant at 30 days to assess clinical outcomes and at 180 days to ascertain vital status. The primary end point is a composite of all-cause death or recurrent MI through 30 days following randomization. Secondary end points include all-cause mortality at 30 days, recurrent adjudicated MI, and the composite outcome of all-cause mortality, nonfatal recurrent MI, ischemia driven unscheduled coronary revascularization (percutaneous coronary intervention or coronary artery bypass grafting), or readmission to the hospital for ischemic cardiac diagnosis within 30 days. The trial will assess multiple tertiary end points.
Conclusions: The MINT trial will inform RBC transfusion practice in patients with acute MI.
Trial registration: ClinicalTrials.gov NCT02981407.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures JLC: DSMB member for Cerus Corporation project. MMB: DSMB member for Cerus Corporation project. JDA: Research funding MicroPort, Boston Scientific. Advisory Boards Philips, Medtronic. Consulting Abbott, Shockwave, Penumbra, Recor. SGG: Research grant support (eg, steering committee or data and safety monitoring committee) and/or speaker/consulting honoraria (eg, advisory boards) from: Amgen, Anthos Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, CSL Behring, Daiichi-Sankyo/American Regent, Eli Lilly, Esperion, Ferring Pharmaceuticals, HLS Therapeutics, JAMP Pharma, Merck, Novartis, Novo Nordisk A/C, Pendopharm/Pharmascience, Pfizer, Regeneron, Sanofi, Servier, Tolmar Pharmaceuticals, Valeo Pharma; and salary support/honoraria from the Heart and Stroke Foundation of Ontario/University of Toronto (Polo) Chair, Canadian Heart Research Centre and MD Primer, Canadian VIGOUR Centre, Cleveland Clinic Coordinating Centre for Clinical Research, Duke Clinical Research Institute, New York University Clinical Coordinating Centre, PERFUSE Research Institute, TIMI Study Group (Brigham Health). AMG: None. MHB: None. Philippe Gabriel Steg: has received research grants from Bayer, Merck, Sanofi, Servier; has been a speaker or consultant for Amarin, Amgen, AstraZeneca, Bayer, Bristol-Myers-Squibb, Janssen, Lexicon, Merck, Novartis, Novo-Nordisk, PhaseBio, Pfizer, Regeneron, Sanofi, Servier. He is a Senior Associate Editor for Circulation. APD: Consultant Velakor Biotherapeutics Inc. RDL: Grants from Bristol-Myers Squibb, GlaxoSmithKline plc., Medtronic, Pfizer, Bayer, Sanofi; consulting fees from Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Novo Nordisk, GlaxoSmithKline plc., Medtronic, Merck, Pfizer, Portola, Sanofi; and honoraria for lectures from Bristol-Myers Squibb, Pfizer, Daiichi Sankyo, Novo Nordisk, and Bayer. PCH: DSMB member of Cerus Corporation project.
References
-
- WHO. Blood Transfusion. In; 2021.
-
- Cooper HA, Rao SV, Greenberg MD, Rumsey MP, McKenzie M, Alcorn KW, et al. Conservative versus liberal red cell transfusion in acute myocardial infarction (the CRIT Randomized Pilot Study). Am J Cardiol 2011;108(8):1108–11. - PubMed
-
- Carson JL, Guyatt G, Heddle NM, Grossman BJ, Cohn CS, Fung MK, et al. Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage. JAMA 2016;316(19):2025–2035. - PubMed
