

Stopping routine urine screening studies for stroke rehabilitation inpatient admissions
- PMID: 36418069
- PMCID: PMC9685004
- DOI: 10.1136/bmjoq-2022-002052
Stopping routine urine screening studies for stroke rehabilitation inpatient admissions
Abstract
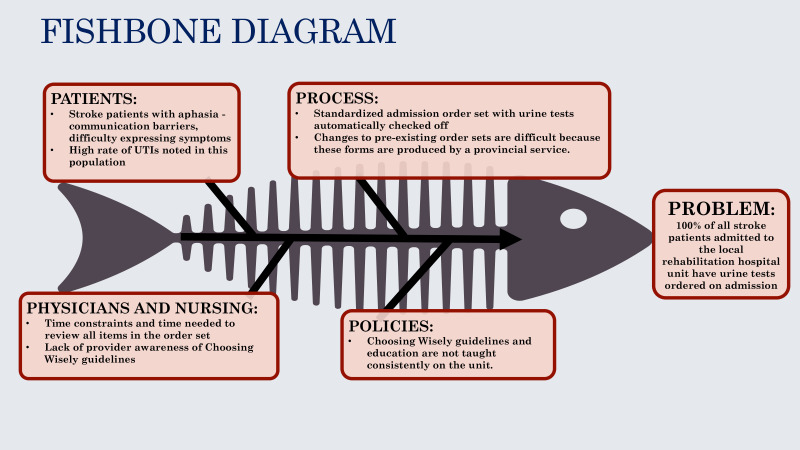
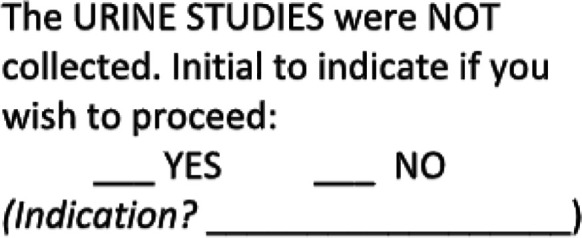
Urine testing on asymptomatic patients is not aligned with guidelines; however, stroke survivors have trouble communicating symptoms, and urinary tract infections (UTIs) are a recognised poststroke complication. All stroke inpatients at a tertiary rehabilitation hospital underwent urine testing on admission. We led a quality improvement (QI) project on one stroke rehabilitation unit aimed to reduce admission urine testing from 100% to 0%. Baseline audit representing 2 weeks of admissions identified 27 of 28 patients had urine tests; however, none required UTI treatment despite 3 positive culture results. Estimated cost of testing was $C675. QI tools identified that a standardised paper-based admission form facilitated automatic urine testing. Project intervention strategies included education, clinicians crossing off urine orders and unit clerks flagging unaddressed orders for reassessment. A chart audit after 4 weeks and prescriber survey after 6 months assessed impact. Postintervention audit (n=23) revealed 1 patient had admission urine tests, 22 orders were crossed out, 1 chart was flagged and estimated testing cost declined from $C675 to $C25. Six urine tests were completed after admission and two patients required UTI treatment. Post 6 months, unit clerks assumed the role to cross out the order on the standardised form, and no patient had routine admission urine testing. There was no clinical benefit in screening for UTIs prior to stroke rehabilitation. This project is a practical example of deadopting a practice promoted by standardised order forms.
Keywords: Diagnosis; Education; Evidence-based medicine; Quality improvement; Rehabilitation.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Nutrition and hydration management among stroke patients in inpatient rehabilitation: a best practice implementation project.JBI Evid Implement. 2021 Mar;19(1):56-67. doi: 10.1097/XEB.0000000000000244. Epub 2020 Jul 17. JBI Evid Implement. 2021. PMID: 33570334
-
The clinical impact of a urinary tract infection management bundle in a tertiary-care teaching hospital.Infect Control Hosp Epidemiol. 2019 Jan;40(1):72-78. doi: 10.1017/ice.2018.276. Epub 2018 Dec 3. Infect Control Hosp Epidemiol. 2019. PMID: 30501661
-
Reassessing the utility of routine urine culture with urodynamics: UTI incidence and risk factors.J Pediatr Urol. 2017 Aug;13(4):372.e1-372.e8. doi: 10.1016/j.jpurol.2017.05.013. Epub 2017 Jun 19. J Pediatr Urol. 2017. PMID: 28713003
-
Recurrent Urinary Tract Infections in Females and the Overlap with Overactive Bladder.Curr Urol Rep. 2018 Sep 13;19(11):94. doi: 10.1007/s11934-018-0839-3. Curr Urol Rep. 2018. PMID: 30215140 Review.
-
Urinary tract infections in older women: a clinical review.JAMA. 2014 Feb 26;311(8):844-54. doi: 10.1001/jama.2014.303. JAMA. 2014. PMID: 24570248 Free PMC article. Review.
References
-
- Hung J-W, Tsay T-H, Chang H-W, et al. . Incidence and risk factors of medical complications during inpatient stroke rehabilitation. Chang Gung Med J 2005;28:31–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical