

Pheochromocytoma Multisystem Crisis Complicated by Severe Acute Pancreatitis
- PMID: 36418097
- PMCID: PMC10372264
- DOI: 10.2169/internalmedicine.0742-22
Pheochromocytoma Multisystem Crisis Complicated by Severe Acute Pancreatitis
Abstract
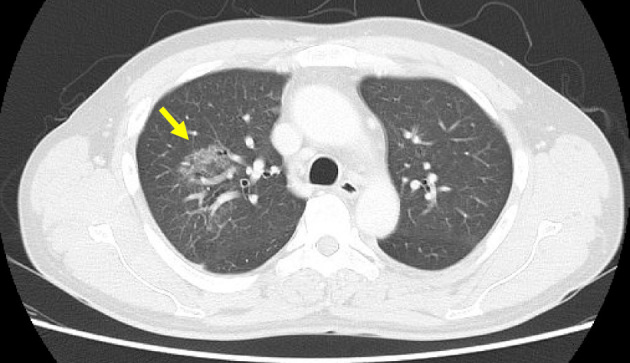
A 43-year-old man developed headache, dizziness, abdominal pain, and vomiting. His blood pressure was 203/121 mmHg, heart rate 122 beats/min, body temperature 39.1°C, and respiratory rate 24/min. He had elevated levels of creatinine at 2.95 mg/dL and lipase at 1,364 U/L as well as an extremely low calcium level at 5.2 mg/dL. Hypertriglyceridemia and hyperglycemia were seen. Chest and abdominal computed tomography showed interstitial pneumonia, severe pancreatitis, and a right adrenal tumor. The patient also developed vertebral artery dissection and medullary infarction. After right adrenalectomy, the patient was diagnosed with pheochromocytoma multisystem crisis (PMC). Acute pancreatitis might augment numerous life-threatening manifestations of PMC.
Keywords: acute pancreatitis; pheochromocytoma multisystem crisis.
Conflict of interest statement
Figures






Similar articles
-
Thyrotoxic and pheochromocytoma multisystem crisis: a case report.J Med Case Rep. 2017 Jun 23;11(1):173. doi: 10.1186/s13256-017-1299-y. J Med Case Rep. 2017. PMID: 28641581 Free PMC article.
-
A case of a composite adrenal medullary tumor of pheochromocytoma and ganglioneuroma masquerading as acute pancreatitis.Korean J Intern Med. 2006 Jun;21(2):141-5. doi: 10.3904/kjim.2006.21.2.141. Korean J Intern Med. 2006. PMID: 16913447 Free PMC article.
-
Pheochromocytoma Multisystem Crisis Behaving Like Interstitial Pneumonia: An Autopsy Case.Intern Med. 2017;56(2):149-152. doi: 10.2169/internalmedicine.56.7449. Epub 2017 Jan 15. Intern Med. 2017. PMID: 28090043 Free PMC article.
-
Pheochromocytoma multisystem crisis treated with emergency surgery: a case report and literature review.BMC Res Notes. 2015 Dec 9;8:758. doi: 10.1186/s13104-015-1738-z. BMC Res Notes. 2015. PMID: 26645353 Free PMC article. Review.
-
Imipramine-provoked paradoxical pheochromocytoma crisis: a case of cardiogenic shock.Am J Emerg Med. 1994 Mar;12(2):190-2. doi: 10.1016/0735-6757(94)90245-3. Am J Emerg Med. 1994. PMID: 8161395 Review.
Cited by
-
A case of simultaneous adrenalectomy and dissection repair with direct sheath placement into the aorta and systematic review of cases with hyperaldosteronism and vascular dissection: a case report.J Med Case Rep. 2025 May 19;19(1):237. doi: 10.1186/s13256-025-05276-1. J Med Case Rep. 2025. PMID: 40390068 Free PMC article.
References
-
- Ando Y, Ono Y, Sano A, Fujita N, Ono S, Tanaka Y. Clinical characteristics and outcomes of pheochromocytoma crisis: a literature review of 200 cases. J Endocrinol Invest 2022 Jul 20. - PubMed
-
- Gan TJ, Miller RF, Webb AR, et al. . Phaeochromocytoma presenting as acute hyperamylasaemia and multiple organ failure. Can J Anaesth 41: 244-247, 1994. - PubMed
-
- Banks PA, Bollen TL, Dervenis C, et al.. Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 62: 102-111, 2013. - PubMed
-
- Takada T, Isaji S, Mayumi T, et al. . JPN clinical practice guidelines 2021 with easy-to-understand explanations for the management of acute pancreatitis. J Hepatobiliary Pancreat Sci 29: 1057-1083, 2022. - PubMed