

Noninvasive Assessment of Human Epidermal Growth Factor Receptor 2 (HER2) in Esophagogastric Cancer Using 89Zr-Trastuzumab PET: A Pilot Study
- PMID: 36418168
- PMCID: PMC10152123
- DOI: 10.2967/jnumed.122.264470
Noninvasive Assessment of Human Epidermal Growth Factor Receptor 2 (HER2) in Esophagogastric Cancer Using 89Zr-Trastuzumab PET: A Pilot Study
Abstract
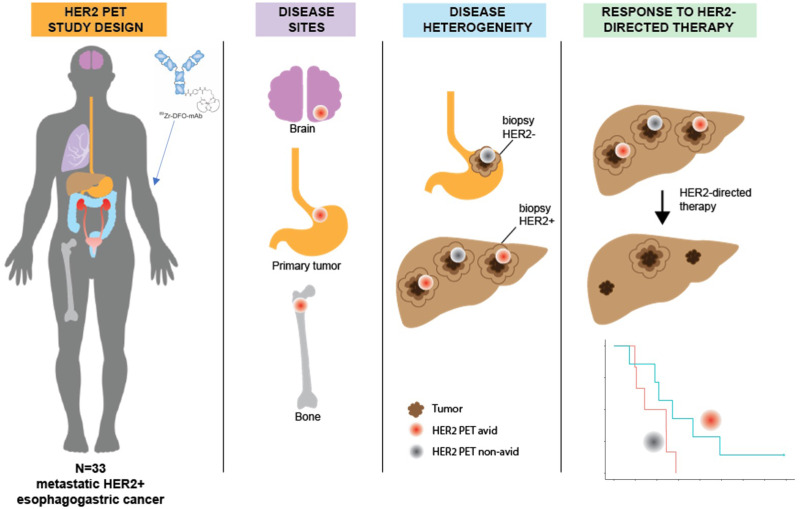
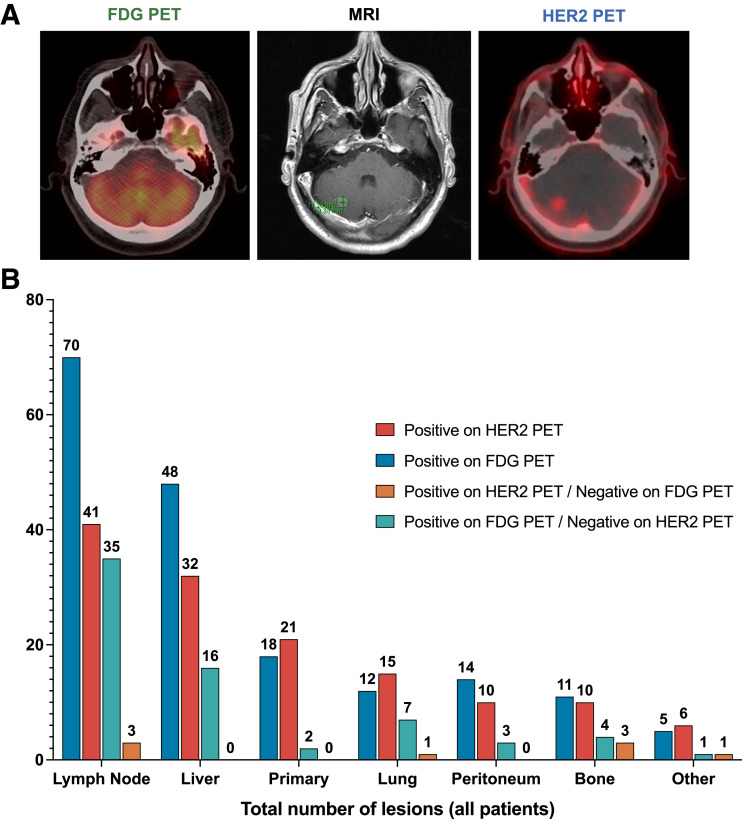
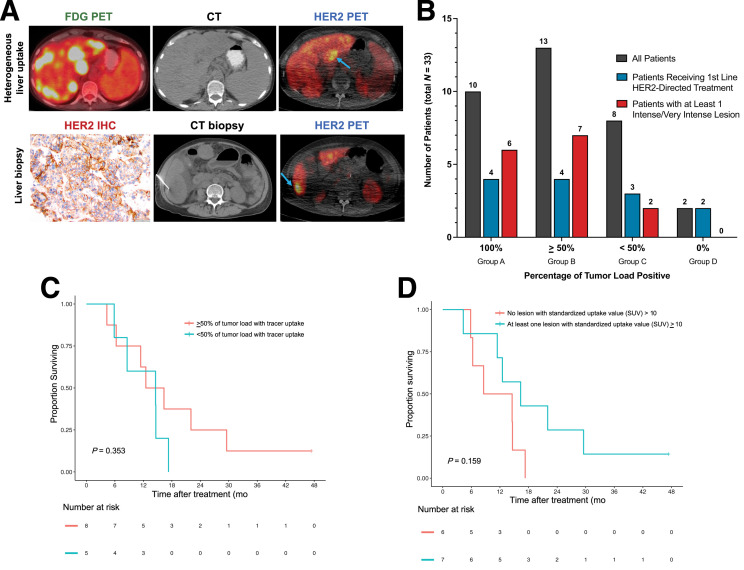
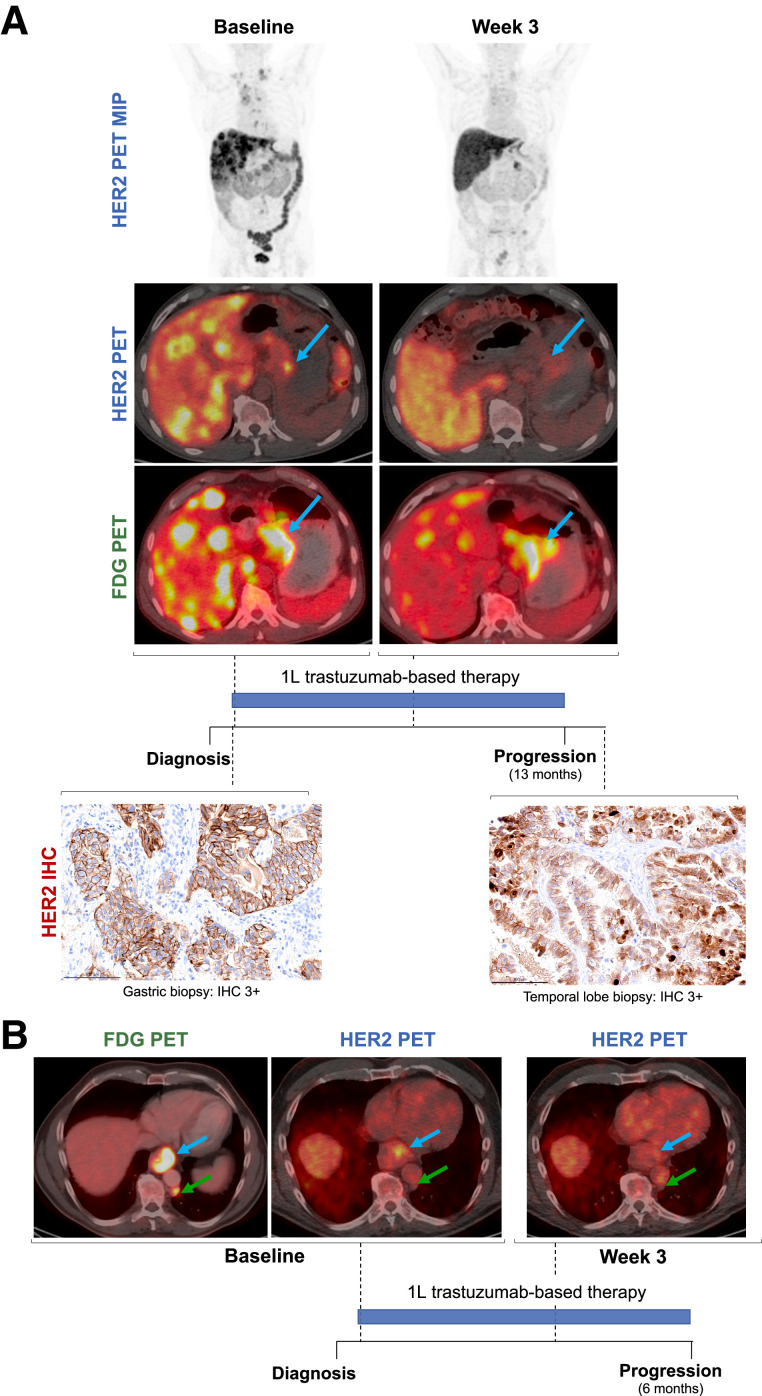
Variations in human epidermal growth factor receptor 2 (HER2) expression between the primary tumor and metastases may contribute to drug resistance in HER2-positive (HER2+) metastatic esophagogastric cancer (mEGC). 89Zr-trastuzumab PET (HER2 PET) holds promise for noninvasive assessment of variations in HER2 expression and target engagement. The aim of this study was to describe HER2 PET findings in patients with mEGC. Methods: Patients with HER2+ mEGC were imaged with HER2 PET, 18F-FDG PET, and CT. Lesions were annotated using measurements (on CT) and maximum SUVs (on HER2 PET). Correlation of visualized disease burden among imaging modalities with clinical and pathologic characteristics was performed. Results: Thirty-three patients with HER2+ mEGC were imaged with HER2 PET and CT (12% esophageal, 64% gastroesophageal junction, and 24% gastric adenocarcinoma), 26 of whom were also imaged with 18F-FDG PET. More lesions were identified on 18F-FDG PET (median, 7 [range, 1-14]) than HER2 PET (median, 4 [range, 0-11]). Of the 8 lesions identified on HER2 but not on 18F-FDG PET, 3 (38%) were in bone and 1 was in the brain. Of the 68 lesions identified on 18F-FDG but not on HER2 PET, 4 (6%) were in bone and the remainder were in the lymph nodes (35, 51%) and liver (16, 24%). Of the 33 total patients, 23 (70%) were HER2 imaging-positive (≥50% of tumor load positive). Only 10 patients had 100% of the tumor load positive; 2 had 0% positive. When only patients receiving HER2-directed therapy as first-line treatment were considered (n = 13), median progression-free survival (PFS) therapy was not significantly different between HER2 imaging-positive and -negative patients. Median PFS for patients with at least 1 intense or very intense lesion (SUV ≥ 10) was 16 (95% CI: 11-not reached) mo (n = 7), compared with 12 (95% CI: 6.3-not reached) mo for patients without an intense or very intense lesion (n = 6) (P = 0.35). Conclusion: HER2 PET may identify heterogeneity of HER2 expression and allow assessment of lesions throughout the entire body. A potential application of HER2 PET is noninvasive evaluation of HER2 status including assessment of intrapatient disease heterogeneity not captured by standard imaging or single-site biopsies.
Keywords: HER2 PET; HER2 heterogeneity; esophageal adenocarcinoma; gastric adenocarcinoma; trastuzumab.
© 2023 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Reichelt U, Duesedau P, Tsourlakis MC, et al. . Frequent homogeneous HER-2 amplification in primary and metastatic adenocarcinoma of the esophagus. Mod Pathol. 2007;20:120–129. - PubMed
-
- Janjigian YY, Werner D, Pauligk C, et al. . Prognosis of metastatic gastric and gastroesophageal junction cancer by HER2 status: a European and USA International collaborative analysis. Ann Oncol. 2012;23:2656–2662. - PubMed
-
- Schoppmann SF, Jesch B, Friedrich J, et al. . Expression of Her-2 in carcinomas of the esophagus. Am J Surg Pathol. 2010;34:1868–1873. - PubMed
-
- Bang YJ, Van Cutsem E, Feyereislova A, et al. . Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet. 2010;376:687–697. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous