

Postpartum pelvic floor muscle training, levator ani avulsion and levator hiatus area: a randomized trial
- PMID: 36418566
- PMCID: PMC9870957
- DOI: 10.1007/s00192-022-05406-z
Postpartum pelvic floor muscle training, levator ani avulsion and levator hiatus area: a randomized trial
Abstract
Introduction and hypothesis: Vaginal delivery may lead to tearing of the levator ani (LA) muscle from its bony insertions (complete LA avulsion) and increased levator hiatus (LH) area, both risk factors for pelvic floor dysfunctions. Early active rehabilitation is standard treatment after musculo-skeletal injury. We hypothesized that pelvic floor muscle training (PFMT) early postpartum would reduce the presence of LA avulsions and reduce LH area.
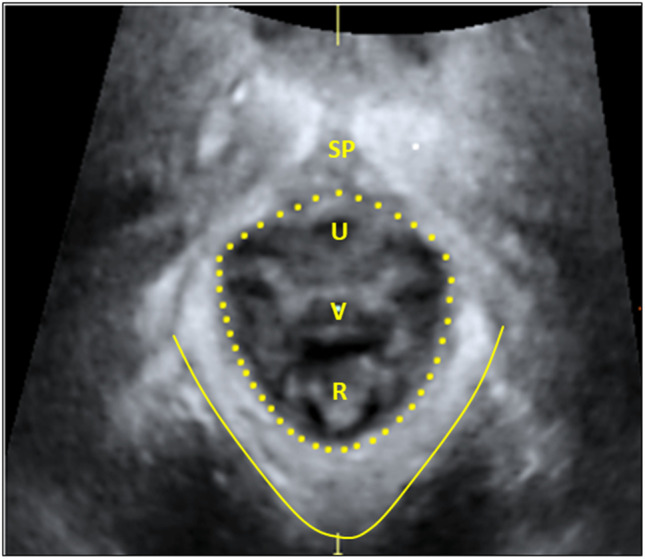
Methods: We carried out a planned secondary analysis from a randomized controlled study. Primiparous women (n=175) giving birth vaginally were included 6 weeks postpartum, stratified on complete LA avulsion, and thereafter randomized to PFMT or control. The training participants (n=87) attended a supervised PFMT class once a week and performed home-based PFMT daily for 16 weeks. The control participants (n=88) received no intervention. Presence of complete LA avulsion, LH area at rest, maximal contraction, and maximal Valsalva maneuver were assessed by transperineal ultrasound. Between-group comparisons were analyzed by analysis of covariance for continuous data, and relative risk (RR) for categorical data.
Results: Six months postpartum, the number of women who had complete LA avulsion was reduced from 27 to 14 within the PFMT group (44% reduction) and from 28 to 17 within the control group (39% reduction). The between-group difference was not significant, RR 0.85 (95% CI 0.53 to 1.37). Further, no significant between-group differences were found for LH area at rest, during contraction, or Valsalva.
Conclusions: Supervised PFMT class combined with home exercise early postpartum did not reduce the presence of complete LA avulsion or LH area more than natural remission.
Keywords: Levator ani muscle avulsion; Levator hiatus area; Physical therapy; Postpartum pelvic floor muscle training; Vaginal delivery.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
