

Inequity in access to continuous glucose monitoring and health outcomes in paediatric diabetes, a case for national continuous glucose monitoring funding: A cross-sectional population study of children with type 1 diabetes in New Zealand
- PMID: 36419466
- PMCID: PMC9676142
- DOI: 10.1016/j.lanwpc.2022.100644
Inequity in access to continuous glucose monitoring and health outcomes in paediatric diabetes, a case for national continuous glucose monitoring funding: A cross-sectional population study of children with type 1 diabetes in New Zealand
Abstract
Background: Continuous glucose monitoring (CGM) improves glycaemia for people affected by type 1 diabetes (T1D), but is not funded in Aotearoa/New Zealand. This study explores the impact of non-funded CGM on equity of access and associated glycaemic outcomes.
Methods: Cross-sectional population-based study collected socio-demographic (age, gender, prioritised ethnicity, socioeconomic status) and clinical data from all regional diabetes centres in New Zealand with children <15 years with T1D as of 1st October 2021. De-identified data were obtained from existing databases or chart review. Outcomes compared socio-demographic characteristics between those using all forms of CGM and self-monitoring of blood glucose (SMBG), and association with HbA1c.
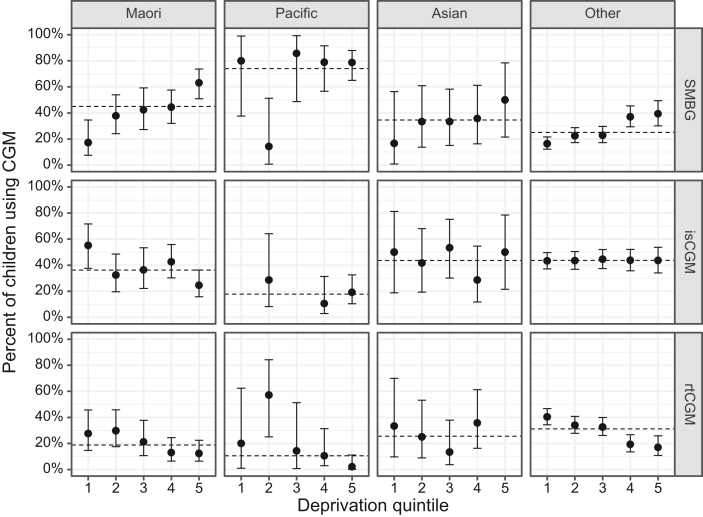
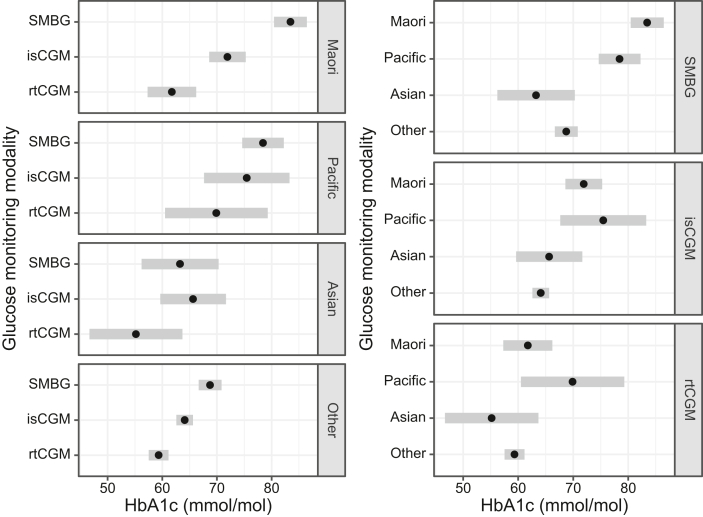
Findings: 1209 eligible children were evaluated: 70.2% European, 18.1% Māori, 7.1% Pacific, 4.6% Asian, with even distribution across socioeconomic quintiles. Median HbA1c was 64 mmol/mol (8.0%), 40.2% utilised intermittently scanned (is)CGM, and 27.2% real-time (rt)CGM. CGM utilisation was lowest with Pacific ethnicity (38% lower than Māori) and the most deprived socioeconomic quintiles (quintile 5 vs. 1 adjusted RR 0.69; 95% CI, 0.57 to 0.84). CGM use was associated with regional diabetes centre (P < 0.001). The impact of CGM use on HbA1c differed by ethnicity: Māori children had the greatest difference in HbA1c between SMBG and rtCGM (adjusted difference -15.3 mmol/mol; 95% CI, -21.5 to -9.1), with less pronounced differences seen with other ethnicities.
Interpretation: Inequities in CGM use exist based on prioritised ethnicity and socioeconomic status. Importantly, CGM was independently associated with lower HbA1c, suggesting that lack of CGM funding contributes to health disparity in children with T1D.
Funding: Australasian Paediatric Endocrine Group (APEG), Canterbury Medical Research Foundation, Starship Foundation.
Keywords: Continuous glucose monitoring; Diabetes technology; Disparity; Equity; Paediatrics; Type 1 diabetes.
© 2022 The Authors.
Conflict of interest statement
MB has received research grants from the 10.13039/501100001505Health Research Council of New Zealand and 10.13039/501100020473Australasian Paediatric Endocrine Group. HD has no conflicts of interest to declare. CJ, RP, BW, and EW are named investigators and MdB is a named Principal Investigator on the Australasian Paediatric Endocrine Group grant provided for this study. RP has received research grants from the 10.13039/501100001505Health Research Council of New Zealand, Lotteries, 10.13039/501100001515Cure Kids, 10.13039/100011367Royal New Zealand College of General Practitioners, 10.13039/501100001529Waikato Medical Research Foundation, and 10.13039/100010061University of Waikato. RP has received educational honoraria from Eli Lilly, Boehringer Ingelheim, Novo Nordisk, Astra Zeneca, Sanofi, Novartis, and Blue Horizons. RP is on the Eli Lilly New Zealand Medical Advisory Board. RP is an Executive Member of the New Zealand Society for the Study of Diabetes, Ministry of Health Expert Diabetes Advisory Group Member, Royal Australasian College of Physicians Adult General Medicine Committee member, and Convener of the New Zealand Diabetes Guidance Group. RP was previously president of the New Zealand Society of Endocrinology. BW has received research grants and equipment from Medtronic, 10.13039/100015769Dexcom, and iSENS. JW is a named investigator on research grants received from the 10.13039/501100001505Health Research Council of New Zealand, 10.13039/501100001530Canterbury Medical Research Foundation, 10.13039/100015769Dexcom, 10.13039/501100001563Otago Medical Research Foundation, National Science Challenge, the 10.13039/100014144Rea Charitable Trust. JW has had research contracts with the Ministry of Health, New Zealand, and the Health Quality and Safety Commission, New Zealand with payments made to his employer/institution, the University of Otago. YA is Chairperson of the Tamariki Pakari Child Health and Wellbeing Trust. MdB has received research grants from 10.13039/100015769Dexcom and Medtronic, and research equipment from Dexcom, Medtronic, and Ypsomed. MdB has received honoraria from Medtronic, Ypsomed, and Dexcom.
Figures
Comment in
-
The need for transparent reporting of ethnicity in health research.N Z Med J. 2024 Sep 27;137(1603):147-149. doi: 10.26635/6965.6686. N Z Med J. 2024. PMID: 39326026 No abstract available.
Similar articles
-
Emergent inequity of glycaemic metrics for Māori children with type 1 diabetes is negated by early use of continuous glucose monitoring.N Z Med J. 2024 Jul 5;137(1598):14-21. doi: 10.26635/6965.6470. N Z Med J. 2024. PMID: 38963927
-
Technology usage and glycaemic outcomes in a single tertiary centre with an ethnically diverse and socioeconomically deprived cohort of children with type 1 diabetes mellitus.Front Clin Diabetes Healthc. 2025 Jan 9;5:1417287. doi: 10.3389/fcdhc.2024.1417287. eCollection 2024. Front Clin Diabetes Healthc. 2025. PMID: 39850852 Free PMC article.
-
Diabetes technology and treatments in the paediatric age group.Int J Clin Pract Suppl. 2011 Feb;(170):76-82. doi: 10.1111/j.1742-1241.2010.02582.x. Int J Clin Pract Suppl. 2011. PMID: 21323816 Review.
-
Real-world glycaemic outcomes in adult persons with type 1 diabetes using a real-time continuous glucose monitor compared to an intermittently scanned glucose monitor: A retrospective observational study from the Canadian LMC diabetes registry (REAL-CGM-T1D).Diabet Med. 2022 Nov;39(11):e14937. doi: 10.1111/dme.14937. Epub 2022 Sep 6. Diabet Med. 2022. PMID: 36065977 Free PMC article.
-
Comparing the glycaemic outcomes between real-time continuous glucose monitoring (rt-CGM) and intermittently scanned continuous glucose monitoring (isCGM) among adults and children with type 1 diabetes: A systematic review and meta-analysis of randomized controlled trials.Diabet Med. 2024 Mar;41(3):e15280. doi: 10.1111/dme.15280. Epub 2024 Jan 10. Diabet Med. 2024. PMID: 38197238
Cited by
-
Area deprivation and demographic factors associated with diabetes technology use in adults with type 1 diabetes in Germany.Front Endocrinol (Lausanne). 2023 Aug 1;14:1191138. doi: 10.3389/fendo.2023.1191138. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37600703 Free PMC article.
-
Characteristics of Children, Youth, and Young Adults With Diabetes: A Cross-Sectional Study in New Zealand Aotearoa.J Diabetes Res. 2024 Dec 10;2024:9968545. doi: 10.1155/jdr/9968545. eCollection 2024. J Diabetes Res. 2024. PMID: 39691822 Free PMC article.
-
International Society for Pediatric and Adolescent Diabetes Clinical Practice Consensus Guidelines 2024: Glycemic Targets.Horm Res Paediatr. 2024;97(6):546-554. doi: 10.1159/000543266. Epub 2024 Dec 19. Horm Res Paediatr. 2024. PMID: 39701064 Free PMC article.
-
Impact of Continuous Glucose Monitoring on Hemoglobin A1c and Height Trends in Latin American Children with Type 1 Diabetes Onset over 3 Years: A Multicenter Study.J Pediatr Clin Pract. 2024 Oct 15;14:200130. doi: 10.1016/j.jpedcp.2024.200130. eCollection 2024 Dec. J Pediatr Clin Pract. 2024. PMID: 39639861 Free PMC article.
-
Predictors of glycaemic improvement in children and young adults with type 1 diabetes and very elevated HbA1c using the MiniMed 780G system.Diabetes Obes Metab. 2025 Apr;27(4):2138-2146. doi: 10.1111/dom.16210. Epub 2025 Jan 20. Diabetes Obes Metab. 2025. PMID: 39831344 Free PMC article.
References
-
- Cardona-Hernandez R., Schwandt A., Alkandari H., et al. Glycemic outcome associated with insulin pump and glucose sensor use in children and adolescents with type 1 diabetes. Data from the international pediatric registry SWEET. Diabetes Care. 2021;44(5):1176–1184. - PubMed
-
- Champakanath A., Akturk H.K., Alonso G.T., Snell-Bergeon J.K., Shah V.N. Continuous glucose monitoring initiation within first year of type 1 diabetes diagnosis is associated with improved glycemic outcomes: 7-year follow-up study. Diabetes Care. 2022;45(3):750–753. - PubMed
LinkOut - more resources
Full Text Sources
