

Oxidative stress markers-driven prognostic model to predict post-discharge mortality in heart failure with reduced ejection fraction
- PMID: 36419488
- PMCID: PMC9676261
- DOI: 10.3389/fcvm.2022.1017673
Oxidative stress markers-driven prognostic model to predict post-discharge mortality in heart failure with reduced ejection fraction
Abstract
Background: Current predictive models based on biomarkers reflective of different pathways of heart failure with reduced ejection fraction (HFrEF) pathogenesis constitute a useful tool for predicting death risk among HFrEF patients. The purpose of the study was to develop a new predictive model for post-discharge mortality risk among HFrEF patients, based on a combination of clinical patients' characteristics, N-terminal pro-B-type Natriuretic peptide (NT-proBNP) and oxidative stress markers as a potentially valuable tool for routine clinical practice.
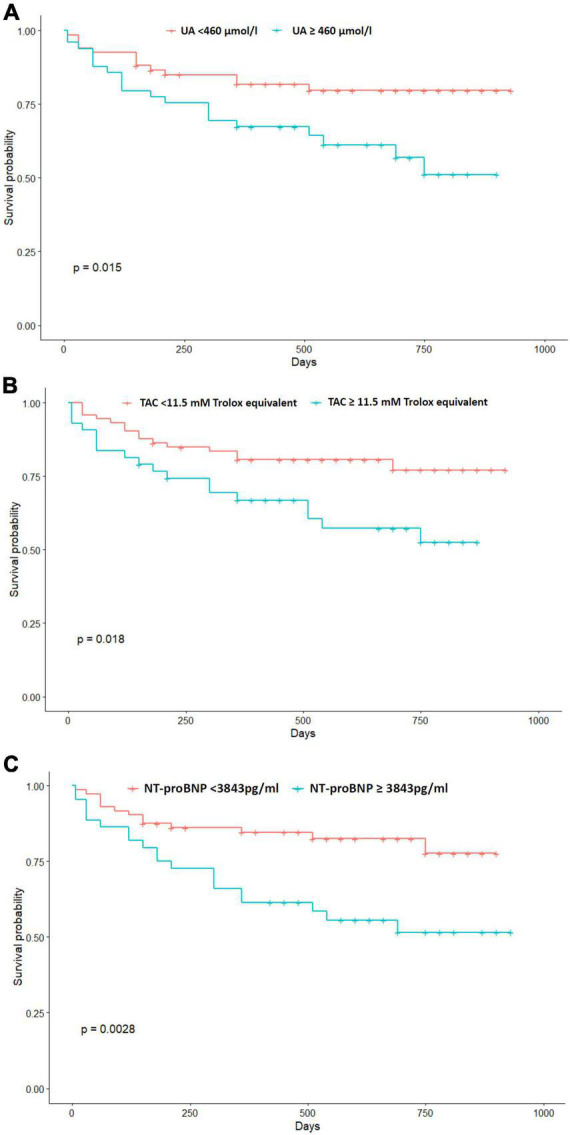
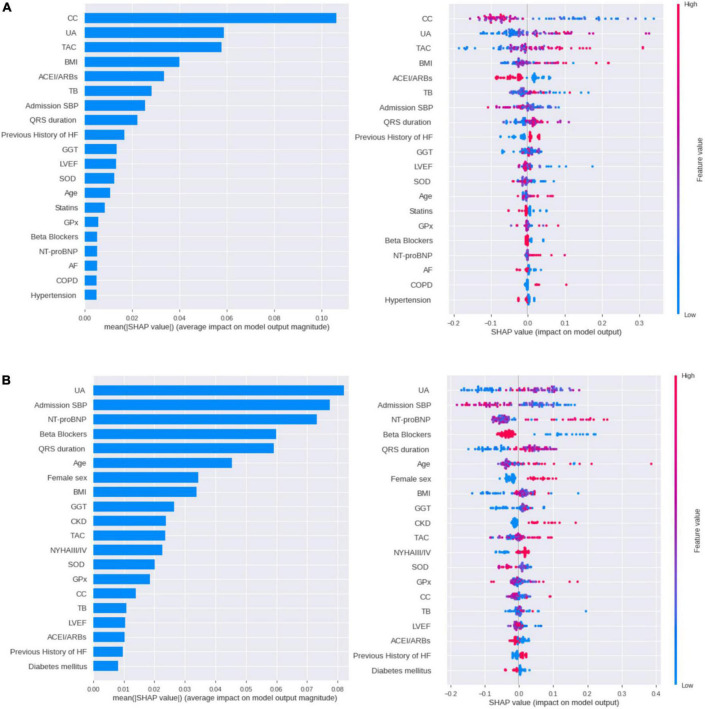
Methods: 116 patients with stable HFrEF were recruited in a prospective single-center study. Plasma levels of NT-proBNP and oxidative stress markers [superoxide dismutase (SOD), glutathione peroxidase (GPX), uric acid (UA), total bilirubin (TB), gamma-glutamyl transferase (GGT) and total antioxidant capacity (TAC)] were measured in the stable predischarge condition. Generalized linear model (GLM), random forest and extreme gradient boosting models were developed to predict post-discharge mortality risk using clinical and laboratory data. Through comprehensive evaluation, the most performant model was selected.
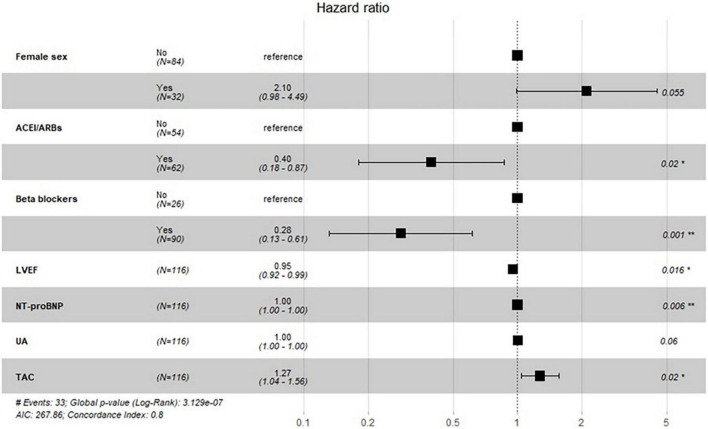
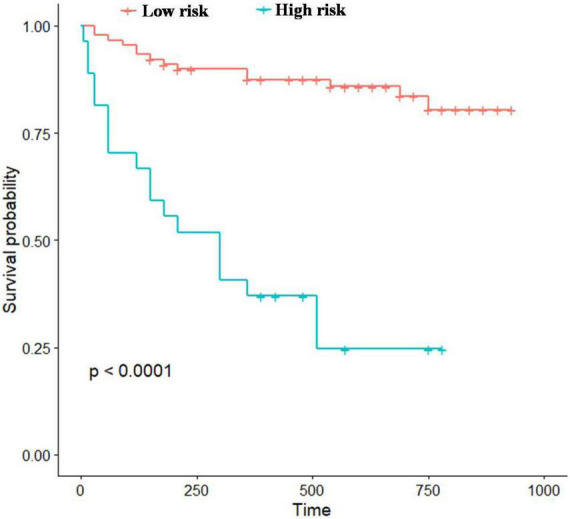
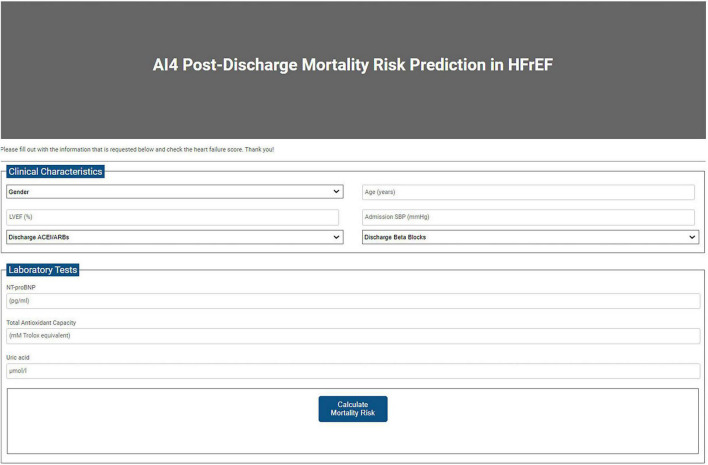
Results: During a median follow-up of 525 days (7-930), 33 (28%) patients died. Among the three created models, the GLM presented the best performance for post-discharge death prediction in HFrEF. The predictors included in the GLM model were age, female sex, beta blockers, NT-proBNP, left ventricular ejection fraction (LVEF), TAC levels, admission systolic blood pressure (SBP), angiotensin-converting enzyme inhibitors/angiotensin receptor II blockers (ACEI/ARBs) and UA levels. Our model had a good discriminatory power for post-discharge mortality [The area under the curve (AUC) = 74.5%]. Based on the retained model, an online calculator was developed to allow the identification of patients with heightened post-discharge death risk.
Conclusion: In conclusion, we created a new and simple tool that may allow the identification of patients at heightened post-discharge mortality risk and could assist the treatment decision-making.
Keywords: heart failure; models; mortality; oxidative stress; prediction.
Copyright © 2022 Gtif, Abdelhedi, Ouarda, Bouzid, Charfeddine, Zouari, Abid, Rebai and Kharrat.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Prognostic value of N-terminal B-type natriuretic peptide on all-cause mortality in heart failure patients with preserved ejection fraction].Zhonghua Xin Xue Guan Bing Za Zhi. 2019 Nov 24;47(11):875-881. doi: 10.3760/cma.j.issn.0253-3758.2019.11.005. Zhonghua Xin Xue Guan Bing Za Zhi. 2019. PMID: 31744276 Chinese.
-
NT-proBNP Response to Sacubitril/Valsartan in Hospitalized Heart Failure Patients With Reduced Ejection Fraction: TRANSITION Study.JACC Heart Fail. 2020 Oct;8(10):822-833. doi: 10.1016/j.jchf.2020.05.012. Epub 2020 Aug 12. JACC Heart Fail. 2020. PMID: 32800508
-
Prognosis and NT-proBNP in heart failure patients with preserved versus reduced ejection fraction.Heart. 2019 Aug;105(15):1182-1189. doi: 10.1136/heartjnl-2018-314173. Epub 2019 Apr 8. Heart. 2019. PMID: 30962192 Free PMC article.
-
The effect of Sacubitril/Valsartan on cardiac function and cardiac remodeling in patients with heart failure with reduced ejection fraction.Ann Palliat Med. 2021 Aug;10(8):8684-8691. doi: 10.21037/apm-21-157. Ann Palliat Med. 2021. PMID: 34488357
-
Novel biomarker-driven prognostic models to predict morbidity and mortality in chronic heart failure: the EMPEROR-Reduced trial.Eur Heart J. 2021 Nov 14;42(43):4455-4464. doi: 10.1093/eurheartj/ehab579. Eur Heart J. 2021. PMID: 34423361 Free PMC article.
Cited by
-
Oxidative Stress Markers and Prediction of Severity With a Machine Learning Approach in Hospitalized Patients With COVID-19 and Severe Lung Disease: Observational, Retrospective, Single-Center Feasibility Study.JMIR Form Res. 2025 Apr 11;9:e66509. doi: 10.2196/66509. JMIR Form Res. 2025. PMID: 40215478 Free PMC article.
-
Association between TyG-BMI and early-onset hypertension: evidence from NHANES.Sci Rep. 2025 Mar 12;15(1):8595. doi: 10.1038/s41598-025-92159-6. Sci Rep. 2025. PMID: 40074808 Free PMC article.
-
Global trends in research on oxidative stress related to heart failure from 2012 to 2021: a bibliometric analysis and suggestion to researchers.Ann Transl Med. 2023 Jan 31;11(2):54. doi: 10.21037/atm-22-6573. Ann Transl Med. 2023. PMID: 36819531 Free PMC article.
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. (2020) 5:15–15. 10.21037/amj.2020.03.03 - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous