

Predictive Performance of the NEWS‒Lactate and NEWS Towards Mortality or Need for Critical Care Among Patients with Suspicion of Sepsis in the Emergency Department: A Prospective Observational Study
- PMID: 36419573
- PMCID: PMC9677920
- DOI: 10.2147/OAEM.S382752
Predictive Performance of the NEWS‒Lactate and NEWS Towards Mortality or Need for Critical Care Among Patients with Suspicion of Sepsis in the Emergency Department: A Prospective Observational Study
Abstract
Objective: We aimed to evaluate the National Early Warning Score‒Lactate (NEWS‒L) and NEWS to predict 24-hour mortality as the primary outcome. The secondary outcomes were to predict 48-hour, 28-day, and in-hospital mortality rates, and the need for critical care in patient with suspicion of sepsis at the emergency department (ED).
Methods: A prospective observational study was performed in patients aged ≥18 years diagnosed with sepsis in the ED from March to November 2021. Area under the receiver operating characteristic curve (AUROC) analyses determined the predictive values of NEWS and NEWS‒L for 24-hour mortality.
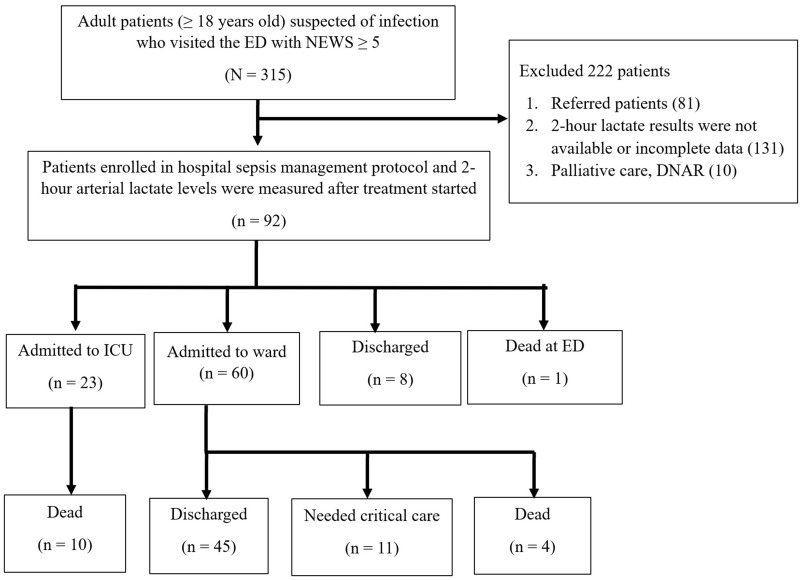
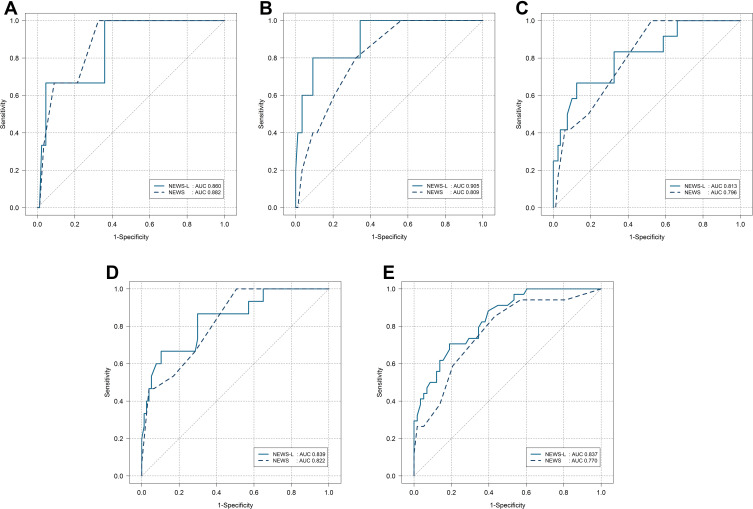
Results: Ninety-two patients were enrolled (mean age 68 years, 48 [52.2%] males). Three (3.2%) patients died within 24 hours and 34 (36.9%) patients needed critical care during the ED stay. The median (interquartile range) NEWS and NEWS-L results were higher in the 24-hour non-survivors versus survivors: 12 (10.5, 12.5) versus 8 (6, 9) (p = 0.024) and 18.7 (15.2, 19.1) versus 10.6 (8.9, 13) (p = 0.036), respectively. The adjusted odds ratio (aOR) was 1.22 for the primary outcome as the NEWS-L increased by 1 unit without statistical significance (p = 0.228). The aOR values for the secondary outcomes ranged from 1.34 to 1.67 with statistical significance. A NEWS-L of 11 and a NEWS of 12 predicted 24-hour mortality with sensitivities/specificities of 100%/56% and 67%/91%, respectively. The AUROC values of NEWS-L for mortality at 24 hours, 48 hours, 28 days, and in-hospital patients, and the need for critical care were 0.860, 0.905, 0.813, 0.839, and 0.837, respectively.
Conclusion: NEWS-L is an accurate predictor for 24-hour mortality in septic patients in the ED. NEWS‒L performed better than NEWS for each outcome. NEWS‒L demonstrated good to excellent performance and was accurate in predicting sepsis related to adverse outcomes.
Keywords: NEWS; NEWS-lactate; National Early Warning Score; mortality; need for critical care; sepsis.
© 2022 Dadeh and Kulparat.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Predictive value of the National Early Warning Score-Lactate for mortality and the need for critical care among general emergency department patients.J Crit Care. 2016 Dec;36:60-68. doi: 10.1016/j.jcrc.2016.06.016. Epub 2016 Jun 29. J Crit Care. 2016. PMID: 27546749
-
Early clinical outcome prediction based on the initial National Early Warning Score + Lactate (News+L) Score among adult emergency department patients.Emerg Med J. 2023 Jun;40(6):444-450. doi: 10.1136/emermed-2022-212654. Emerg Med J. 2023. PMID: 37220969
-
The utility of the rapid emergency medicine score (REMS) compared with SIRS, qSOFA and NEWS for Predicting in-hospital Mortality among Patients with suspicion of Sepsis in an emergency department.BMC Emerg Med. 2021 Jan 7;21(1):2. doi: 10.1186/s12873-020-00396-x. BMC Emerg Med. 2021. PMID: 33413139 Free PMC article.
-
Comparison of qSOFA and Hospital Early Warning Scores for prognosis in suspected sepsis in emergency department patients: a systematic review.Emerg Med J. 2022 Apr;39(4):284-294. doi: 10.1136/emermed-2020-210416. Epub 2021 Aug 17. Emerg Med J. 2022. PMID: 34404680
-
Prognostic value of early warning scores in the emergency department (ED) and acute medical unit (AMU): A narrative review.Eur J Intern Med. 2017 Nov;45:20-31. doi: 10.1016/j.ejim.2017.09.027. Epub 2017 Oct 7. Eur J Intern Med. 2017. PMID: 28993097 Review.
Cited by
-
Adjusting EWS scores for altitude above sea level: is it necessary to predict sepsis mortality in the emergency room?Int J Emerg Med. 2025 Feb 20;18(1):30. doi: 10.1186/s12245-024-00761-8. Int J Emerg Med. 2025. PMID: 39979821 Free PMC article.
-
Evaluating Sepsis Mortality Predictions from the Emergency Department: A Retrospective Cohort Study Comparing qSOFA, the National Early Warning Score, and the International Early Warning Score.J Clin Med. 2025 Jul 9;14(14):4869. doi: 10.3390/jcm14144869. J Clin Med. 2025. PMID: 40725560 Free PMC article.
-
Prehospital qSOFA, mSOFA, and NEWS2 performance for sepsis prediction: A prospective, multi-center, cohort study.Front Med (Lausanne). 2023 Apr 18;10:1149736. doi: 10.3389/fmed.2023.1149736. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37144037 Free PMC article.
-
Prognostic accuracy of lactate and procalcitonin in addition to national early warning score in patients with suspected sepsis - A cross-sectional study in a tertiary care center.Int J Crit Illn Inj Sci. 2024 Oct-Dec;14(4):188-196. doi: 10.4103/ijciis.ijciis_65_24. Epub 2024 Dec 23. Int J Crit Illn Inj Sci. 2024. PMID: 39811035 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
