

Ovarian collision tumor consisting of sclerosing stromal tumor and mature cystic teratoma complicated with Meigs syndrome: A case report
- PMID: 36420070
- PMCID: PMC9647795
- DOI: 10.3892/ol.2022.13563
Ovarian collision tumor consisting of sclerosing stromal tumor and mature cystic teratoma complicated with Meigs syndrome: A case report
Abstract
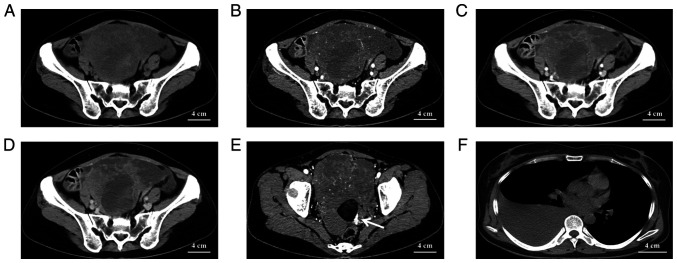
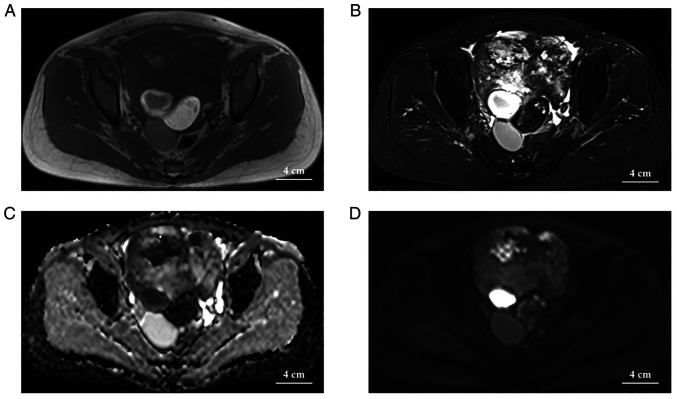
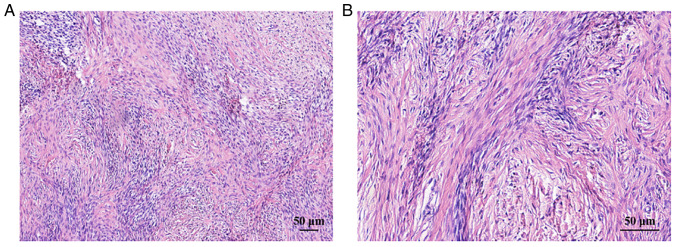
Ovarian collision tumors are uncommon and reports of their radiological appearance are even less frequent. The present study reported the world's first case of an ovarian collision tumor consisting of an ovarian sclerosing stromal tumor and a mature cystic teratoma and its imaging presentation. When a cystic solid ovarian mass combined with ascites and elevated CA125 is encountered it is frequently diagnosed as a malignant tumor, but the present case was a benign tumor. Therefore, when encountering similar cases, clinicians should not limit the diagnosis to malignant tumors to avoid rashly expanding the surgery and causing unnecessary harm to the patient. The combination of computed tomography, magnetic resonance imaging and pathology findings presented in the current study enable radiologists to learn about this disease and further assist clinicians in developing the best treatment plan.
Keywords: case report; computed tomography; magnetic resonance imaging; ovarian collision tumor; sclerosing stromal tumor.
Copyright: © Zhang et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Ovarian Collision Tumor, Massive Mucinous Cystadenoma, and Benign Mature Cystic Teratoma.Cureus. 2021 Jul 6;13(7):e16221. doi: 10.7759/cureus.16221. eCollection 2021 Jul. Cureus. 2021. PMID: 34367821 Free PMC article.
-
Mature Cystic Teratoma with Co-existent Mucinous Cystadenocarcinoma in the same Ovary-A Diagnostic Dilemma.J Clin Diagn Res. 2016 Dec;10(12):ED11-ED13. doi: 10.7860/JCDR/2016/22150.9118. Epub 2016 Dec 1. J Clin Diagn Res. 2016. PMID: 28208869 Free PMC article.
-
Meigs' syndrome with elevated serum cancer antigen 125 levels in a case of ovarian sclerosing stromal tumor.Taiwan J Obstet Gynecol. 2011 Jun;50(2):196-200. doi: 10.1016/j.tjog.2011.01.011. Taiwan J Obstet Gynecol. 2011. PMID: 21791307
-
Diversity of imaging features of ovarian sclerosing stromal tumors on MRI and PET-CT: a case report and literature review.J Ovarian Res. 2018 Dec 20;11(1):101. doi: 10.1186/s13048-018-0473-1. J Ovarian Res. 2018. PMID: 30572921 Free PMC article. Review.
-
A case of death of patient with ovarian fibroma combined with Meigs Syndrome and literature review.Diagn Pathol. 2022 Oct 17;17(1):83. doi: 10.1186/s13000-022-01258-9. Diagn Pathol. 2022. PMID: 36253781 Free PMC article. Review.
Cited by
-
Cystadenofibroma and contralateral collision lesions: A unique ovarian case report.Oncoscience. 2025 Mar 31;12:26-33. doi: 10.18632/oncoscience.616. eCollection 2025. Oncoscience. 2025. PMID: 40165932 Free PMC article.
-
Uterine collision tumor. Case report and review of the literature.Rev Colomb Obstet Ginecol. 2023 Sep 30;74(3):225-236. doi: 10.18597/rcog.4011. Rev Colomb Obstet Ginecol. 2023. PMID: 37937912 Free PMC article. English, Spanish.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous