

Prediction of Noninvasive Ventilation Failure in COVID-19 Patients: When Shall We Stop?
- PMID: 36420242
- PMCID: PMC9679987
- DOI: 10.7759/cureus.30599
Prediction of Noninvasive Ventilation Failure in COVID-19 Patients: When Shall We Stop?
Abstract
Introduction: In coronavirus disease 2019 (COVID-19), there are no tools available for the difficult task of recognizing which patients do not benefit from maintaining respiratory support, such as noninvasive ventilation (NIV). Identifying treatment failure is crucial to provide the best possible care and optimizing resources. Therefore, this study aimed to build a model that predicts NIV failure in patients who did not progress to invasive mechanical ventilation (IMV).
Methods: This retrospective observational study included critical COVID-19 patients treated with NIV who did not progress to IMV. Patients were admitted to a Portuguese tertiary hospital between October 1, 2020, and March 31, 2021. The outcome of interest was NIV failure, defined as COVID-19-related in-hospital death. A binary logistic regression was performed, where the outcome (mortality) was the dependent variable. Using the independent variables of the logistic regression a decision-tree classification model was implemented.
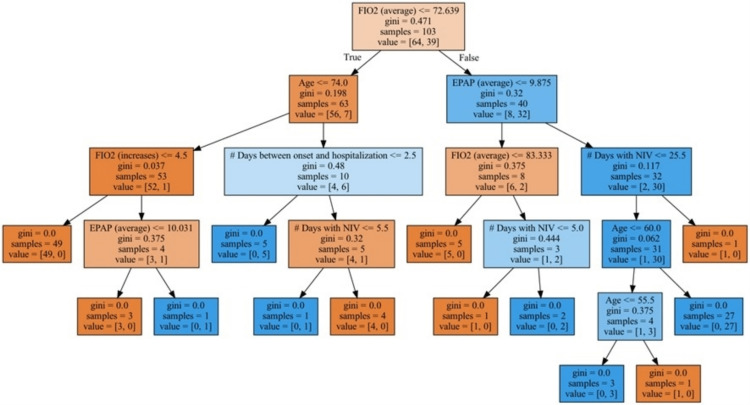
Results: The study sample, composed of 103 patients, had a mean age of 66.3 years (SD=14.9), of which 38.8% (40 patients) were female. Most patients (82.5%) were autonomous for basic activities of daily living. The prediction model was statistically significant with an area under the curve of 0.994 and a precision of 0.950. Higher age, a higher number of days with increases in the fraction of inspired oxygen (FiO2), a higher number of days of maximum expiratory positive airway pressure, a lower number of days on NIV, and a lower number of days from disease onset to hospital admission were, with statistical significance, associated with increased odds of death. A decision-tree classification model was then obtained to achieve the best combination of variables to predict the outcome of interest.
Conclusions: This study presents a model to predict death in COVID-19 patients treated with NIV in patients who did not progress to IMV, based on easily applicable variables that mainly reflect patients' evolution during hospitalization. Along with the decision-tree classification model, these original findings may help clinicians define the best therapeutical approach to each patient, prioritizing life-comforting measures when adequate, and optimizing resources, which is crucial within limited or overloaded healthcare systems. Further research is needed on this subject of treatment failure, not only to understand if these results are reproducible but also, in a broader sense, helping to fill this gap in modern medicine guidelines.
Keywords: covid-19 retro; noninvasive mechanical ventilation; pandemics; prediction tools; resource management; respiratory insufficiency; treatment failure.
Copyright © 2022, Neves da Silva et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Ritchie H, Mathieu E, Rodés-Guirao L, et al. Our World in Data: Coronavirus pandemic (COVID-19) [ Oct; 2021 ]. 2020. https://ourworldindata.org/coronavirus https://ourworldindata.org/coronavirus
-
- COVID-19 Hospitalization And Emergency Department Statistics. [ Oct; 2021 ]. 2020. https://www.cihi.ca/en/covid-19-hospitalization-and-emergency-department... https://www.cihi.ca/en/covid-19-hospitalization-and-emergency-department...
-
- Fair allocation of scarce medical resources in the time of Covid-19. Emanuel EJ, Persad G, Upshur R, et al. N Engl J Med. 2020;382:2049–2055. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous