

Long-Term Pulmonary Dysfunction by Hyperoxia Exposure during Severe Viral Lower Respiratory Tract Infection in Mice
- PMID: 36422586
- PMCID: PMC9696792
- DOI: 10.3390/pathogens11111334
Long-Term Pulmonary Dysfunction by Hyperoxia Exposure during Severe Viral Lower Respiratory Tract Infection in Mice
Abstract
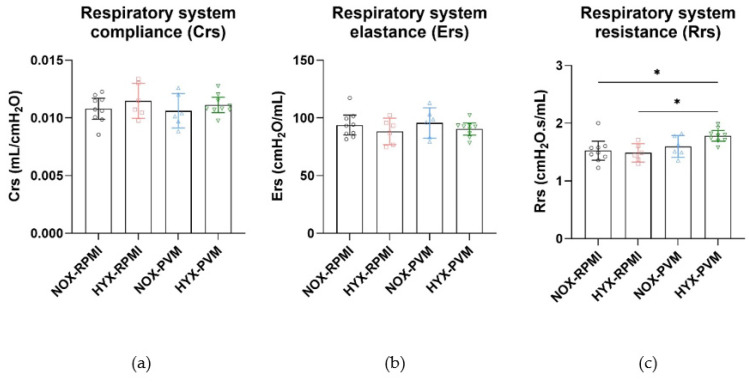
Viral-induced lower respiratory tract infection (LRTI), mainly by respiratory syncytial virus (RSV), causes a major health burden among young children and has been associated with long-term respiratory dysfunction. Children with severe viral LRTI are frequently treated with oxygen therapy, hypothetically posing an additional risk factor for pulmonary sequelae. The main goal of this study was to determine the effect of concurrent hyperoxia exposure during the acute phase of viral LRTI on long-term pulmonary outcome. As an experimental model for severe RSV LRTI in infants, C57Bl/6J mice received an intranasal inoculation with the pneumonia virus of mice J3666 strain at post-natal day 7, and were subsequently exposed to hyperoxia (85% O2) or normoxia (21% O2) from post-natal day 10 to 17 during the acute phase of disease. Long-term outcomes, including lung function and structural development, were assessed 3 weeks post-inoculation at post-natal day 28. Compared to normoxic conditions, hyperoxia exposure in PVM-inoculated mice induced a transient growth arrest without subsequent catchup growth, as well as a long-term increase in airway resistance. This hyperoxia-induced pulmonary dysfunction was not associated with developmental changes to the airway or lung structure. These findings suggest that hyperoxia exposure during viral LRTI at young age may aggravate subsequent long-term pulmonary sequelae. Further research is needed to investigate the specific mechanisms underlying this alteration to pulmonary function.
Keywords: airway resistance; bronchiolitis; hyperoxia; oxygen; pneumovirus; respiratory syncytial viruses; respiratory tract infection.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures






References
-
- Li Y., Wang X., Blau D.M., Caballero M.T., Feikin D.R., Gill C.J., Madhi S.A., Omer S.B., Simoes E.A.F., Campbell H., et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet. 2022;399:2047–2064. doi: 10.1016/S0140-6736(22)00478-0. - DOI - PMC - PubMed
-
- Fauroux B., Simoes E.A.F., Checchia P.A., Paes B., Figueras-Aloy J., Manzoni P., Bont L., Carbonell-Estrany X. The Burden and Long-term Respiratory Morbidity Associated with Respiratory Syncytial Virus Infection in Early Childhood. Infect. Dis. Ther. 2017;6:173–197. doi: 10.1007/s40121-017-0151-4. - DOI - PMC - PubMed
-
- Brunwasser S.M., Snyder B.M., Driscoll A.J., Fell D.B., Savitz D.A., Feikin D.R., Skidmore B., Bhat N., Bont L.J., Dupont W.D., et al. Assessing the strength of evidence for a causal effect of respiratory syncytial virus lower respiratory tract infections on subsequent wheezing illness: A systematic review and meta-analysis. Lancet Respir. Med. 2020;8:795–806. doi: 10.1016/S2213-2600(20)30109-0. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
