

CSF tau microtubule-binding region identifies pathological changes in primary tauopathies
- PMID: 36424467
- PMCID: PMC9800273
- DOI: 10.1038/s41591-022-02075-9
CSF tau microtubule-binding region identifies pathological changes in primary tauopathies
Abstract
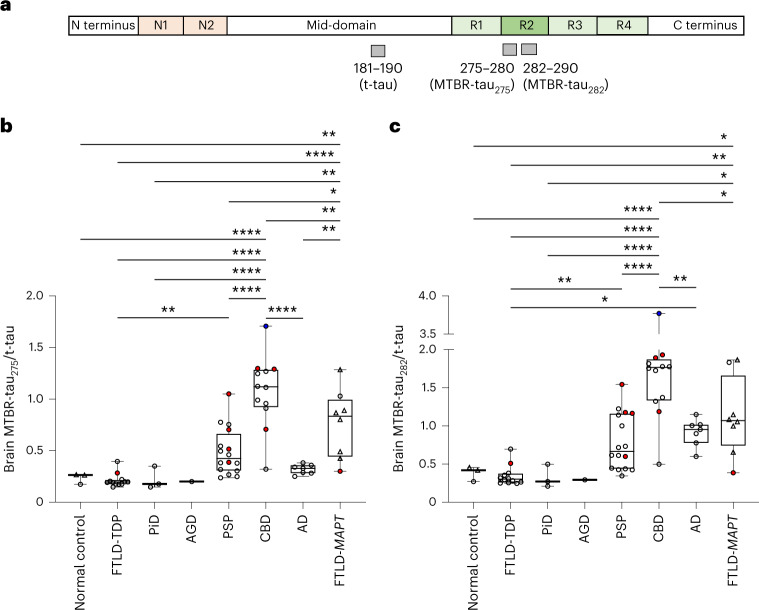
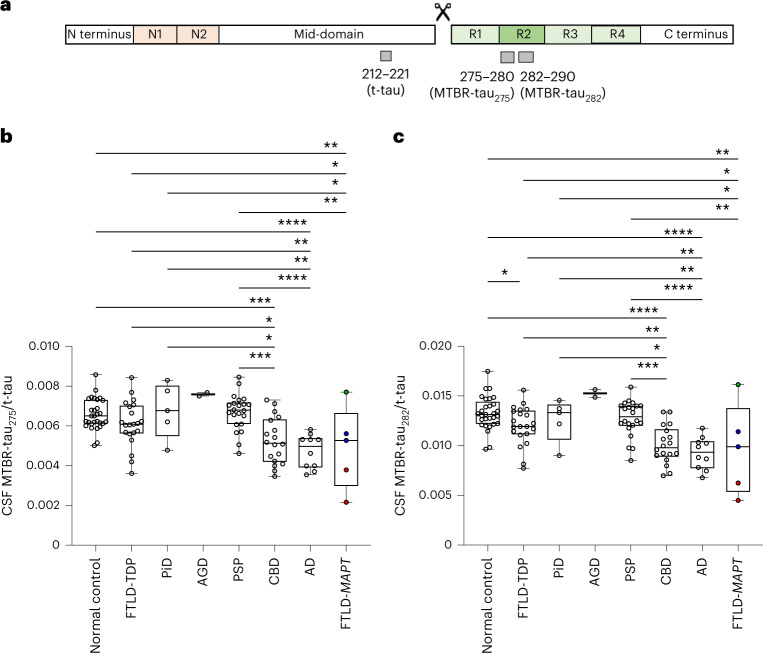
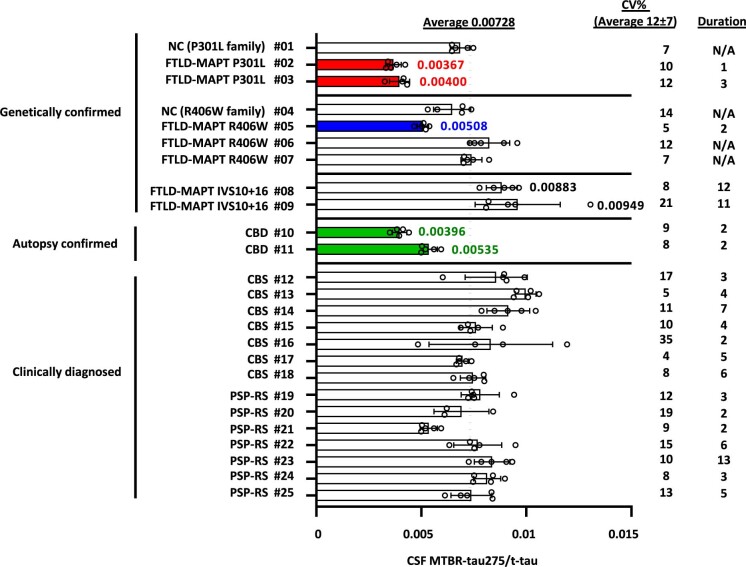
Despite recent advances in fluid biomarker research in Alzheimer's disease (AD), there are no fluid biomarkers or imaging tracers with utility for diagnosis and/or theragnosis available for other tauopathies. Using immunoprecipitation and mass spectrometry, we show that 4 repeat (4R) isoform-specific tau species from microtubule-binding region (MTBR-tau275 and MTBR-tau282) increase in the brains of corticobasal degeneration (CBD), progressive supranuclear palsy (PSP), frontotemporal lobar degeneration (FTLD)-MAPT and AD but decrease inversely in the cerebrospinal fluid (CSF) of CBD, FTLD-MAPT and AD compared to control and other FTLD-tau (for example, Pick's disease). CSF MTBR-tau measures are reproducible in repeated lumbar punctures and can be used to distinguish CBD from control (receiver operating characteristic area under the curve (AUC) = 0.889) and other FTLD-tau, such as PSP (AUC = 0.886). CSF MTBR-tau275 and MTBR-tau282 may represent the first affirmative biomarkers to aid in the diagnosis of primary tauopathies and facilitate clinical trial designs.
© 2022. The Author(s).
Conflict of interest statement
K.H. is an Eisai-sponsored voluntary research associate professor at Washington University and has received salary from Eisai. Washington University and R.J.B. have equity ownership interest in C2N Diagnostics and R.J.B. receives income from C2N Diagnostics for serving on the scientific advisory board. R.J.B., N.R.B., K.H. and C.S. may receive income based on technology (Methods to detect MTBR tau isoforms and use thereof) licensed by Washington University to C2N Diagnostics. R.J.B. has received research funding from Avid Radiopharmaceuticals, Janssen, Roche/Genentech, Eli Lilly, Eisai, Biogen, AbbVie, Bristol Myers Squibb and Novartis. RJB serves on the Roche Gantenerumab Steering Committee as an unpaid member. S.S. has received consultation fees from Techspert.io, Acsel Health and PRECISIONxtract. L.V. has served as a consultant for Retrotope. R.W.P. has received honoraria as an educational speaker for GE Healthcare. B.A.W. has participated or is currently participating in clinical research sponsored by Acadia, Biogen, Global Kinetics, Neurocrine, Prilenia, PTC, Roche, Sage, Vaccinex, Transposon and Triplet Therapeutics. G.S.D.’s research is supported by the NIH (K23AG064029, U01AG057195, U19AG032438), the Alzheimer’s Association and Chan Zuckerberg Initiative. He serves as a consultant for Parabon NanoLabs, as a topic editor (dementia) for DynaMed (EBSCO) and as the Clinical Director of the Anti-NMDA Receptor Encephalitis Foundation (Canada; uncompensated). He is the co-project principal investigator for a clinical trial in anti-
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
- P50 AG023501/AG/NIA NIH HHS/United States
- L30 AG069301/AG/NIA NIH HHS/United States
- U24 AG057437/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- P41 GM103422/GM/NIGMS NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- K12 HD001459/HD/NICHD NIH HHS/United States
- K23 AG064029/AG/NIA NIH HHS/United States
- K08 AG052648/AG/NIA NIH HHS/United States
- R01 NS095773/NS/NINDS NIH HHS/United States
- R56 NS110890/NS/NINDS NIH HHS/United States
- K23 AG073514/AG/NIA NIH HHS/United States
- R01 AG073482/AG/NIA NIH HHS/United States
- P30 AG066444/AG/NIA NIH HHS/United States
- R01 NS065667/NS/NINDS NIH HHS/United States
- K08 NS101118/NS/NINDS NIH HHS/United States
- U19 AG063911/AG/NIA NIH HHS/United States
- P01 AG003991/AG/NIA NIH HHS/United States
- P01 AG026276/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- RF1 NS110890/NS/NINDS NIH HHS/United States
- K01 AG062796/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
