

Cochlear implant-specific risks should be considered, when assessing the quality of life of children and adolescents with hearing loss and cochlear implants-not just cochlear implant-specific benefits-Perspective
- PMID: 36425475
- PMCID: PMC9679369
- DOI: 10.3389/fnins.2022.985230
Cochlear implant-specific risks should be considered, when assessing the quality of life of children and adolescents with hearing loss and cochlear implants-not just cochlear implant-specific benefits-Perspective
Abstract
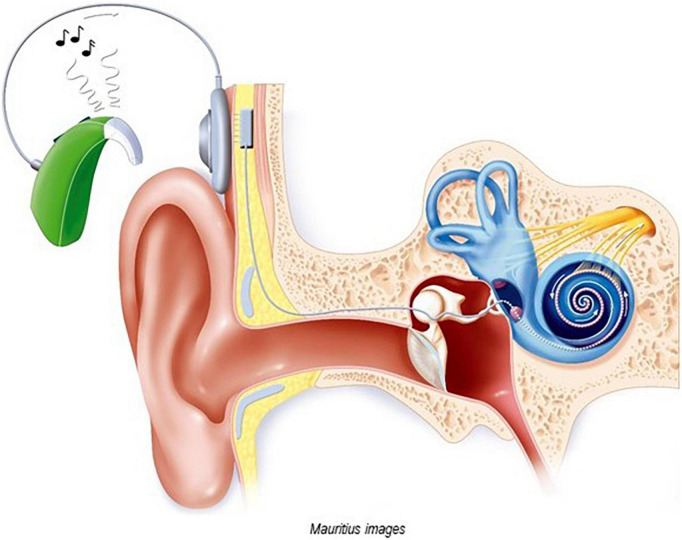
Cochlear implants (CIs) are electronic medical devices that enable hearing in cases where traditional hearing aids are of minimal or no use. Quality of life (QoL) studies of children and adolescents with a CI have so far focused on the CI-specific benefits. However, the CI-specific risks listed by the U.S. Food and Drug Administration have not yet been considered. From this list, medical and device-related complications, lifelong dependency on the implanted device, and neurosecurity risks (CI technology is an interface technology) may be particularly relevant for young CI users. Medical and device-related complications can cause physical discomfort (e.g., fever, pain), as well as functioning problems (e.g., in speech discrimination, social behavior, and mood). In the worst case, reimplantation is required. Clinical experience shows that these complications are perceived as a burden for young CI users. Furthermore, many young patients are worried about possible complications. Additionally, CIs can be at least a temporary burden when children, typically at the age of 8-9 years, realize that they need the CI for life, or when they become peer victims because of their CI. Concerning neurosecurity risks, it is still unknown how young CI recipients perceive them. In summary, CI-specific risks can be perceived as a burden by young CI users that impairs their QoL. Therefore, they should not be ignored. There is an urgent need for studies on this topic, which would not only be important for professionals and parents, but also for the design of CI-specific QoL instruments.
Keywords: CI-specific risks; children and adolescents; cochlear implants; hearing loss; quality of life.
Copyright © 2022 Huber.
Conflict of interest statement
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Restricted Speech Recognition in Noise and Quality of Life of Hearing-Impaired Children and Adolescents With Cochlear Implants - Need for Studies Addressing This Topic With Valid Pediatric Quality of Life Instruments.Front Psychol. 2019 Sep 12;10:2085. doi: 10.3389/fpsyg.2019.02085. eCollection 2019. Front Psychol. 2019. PMID: 31572268 Free PMC article.
-
[Cochlear implant in children: rational, indications and cost/efficacy].Minerva Pediatr. 2013 Jun;65(3):325-39. Minerva Pediatr. 2013. PMID: 23685383 Review. Italian.
-
Quality of Life-CI: Development of an Early Childhood Parent-Proxy and Adolescent Version.Ear Hear. 2021 July/Aug;42(4):1072-1083. doi: 10.1097/AUD.0000000000001004. Ear Hear. 2021. PMID: 33974778 Free PMC article.
-
American parent perspectives on quality of life in pediatric cochlear implant recipients.Ear Hear. 2015 Mar-Apr;36(2):269-78. doi: 10.1097/AUD.0000000000000108. Ear Hear. 2015. PMID: 25377531
-
Systematic Review of Quality of Life Assessments after Cochlear Implantation in Older Adults.Audiol Neurootol. 2021;26(2):61-75. doi: 10.1159/000508433. Epub 2020 Jul 10. Audiol Neurootol. 2021. PMID: 32653882
Cited by
-
Knowledge, attitude, and practice toward cochlear implants among deaf patients who received cochlear implants.Sci Rep. 2024 Feb 23;14(1):4451. doi: 10.1038/s41598-024-55006-8. Sci Rep. 2024. PMID: 38396067 Free PMC article.
References
-
- Archbold S. M., Mark E., Lutman M. E., Gregory S., O’Neill C., Nikolopoulos T. P. (2002). Parents and their deaf child: Their perceptions three years after cochlear implantation. Deaf. Educ. Int. 4 12–40. 10.1179/146431502790560962 - DOI
LinkOut - more resources
Full Text Sources