

This is a preprint.
Acute and Post-Acute COVID-19 Outcomes Among Immunologically Naïve Adults During Delta Versus Omicron Waves
- PMID: 36425923
- PMCID: PMC9685683
- DOI: 10.1101/2022.11.13.22282222
Acute and Post-Acute COVID-19 Outcomes Among Immunologically Naïve Adults During Delta Versus Omicron Waves
Update in
-
Acute and Postacute COVID-19 Outcomes Among Immunologically Naive Adults During Delta vs Omicron Waves.JAMA Netw Open. 2023 Feb 1;6(2):e231181. doi: 10.1001/jamanetworkopen.2023.1181. JAMA Netw Open. 2023. PMID: 36853602 Free PMC article.
Abstract
Importance: The U.S. arrival of the Omicron variant led to a rapid increase in SARS-CoV-2 infections. While numerous studies report characteristics of Omicron infections among vaccinated individuals and/or persons with a prior history of infection, comprehensive data describing infections among immunologically naïve adults is lacking.
Objective: To examine COVID-19 acute and post-acute clinical outcomes among a well-characterized cohort of unvaccinated and previously uninfected adults who contracted SARS-CoV-2 during the Omicron (BA.1/BA.2) surge, and to compare outcomes with infections that occurred during the Delta wave.
Design: A prospective cohort undergoing high-resolution symptom and virologic monitoring between June 2021 and September 2022.
Setting: Multisite recruitment of community-dwelling adults in 8 U.S. states.
Participants: Healthy, unvaccinated adults between 30 to 64 years of age without an immunological history of SARS-CoV-2 who were at high-risk of infection were recruited. Participants were followed for up to 48 weeks, submitting regular COVID-19 symptom surveys and nasal swabs for SARS-CoV-2 PCR testing.
Exposures: Omicron (BA.1/BA.2 lineages) versus Delta SARS-CoV-2 infection, defined as a positive PCR that occurred during a period when the variant represented ≥50% of circulating SARS-CoV-2 variants in the participant's geographic region.
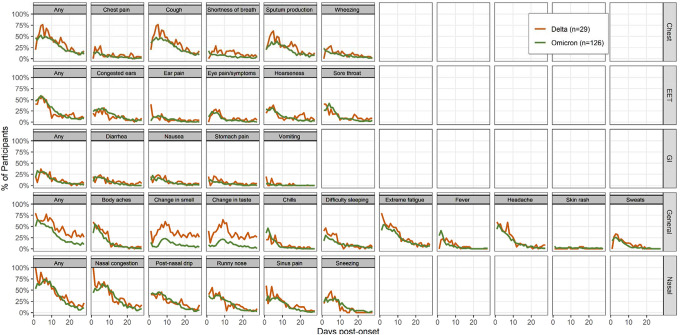
Main outcomes and measures: The main outcomes examined were the prevalence and severity of acute (≤28 days post-onset) and post-acute (≥5 weeks post-onset) symptoms.
Results: Among 274 immunologically naïve participants, 166 (61%) contracted SARS-CoV-2. Of these, 137 (83%) and 29 (17%) infections occurred during the Omicron- and Delta-predominant periods, respectively. Asymptomatic infections occurred among 6.7% (95% CI: 3.1%, 12.3%) of Omicron cases and 0.0% (95% CI: 0.0%, 11.9%) of Delta cases. Healthcare utilization among Omicron cases was 79% (95% CI: 43%, 92%, P =0.001) lower relative to Delta cases. Relative to Delta, Omicron infections also experienced a 56% (95% CI: 26%, 74%, P =0.004) and 79% (95% CI: 54%, 91%, P <0.001) reduction in the risk and rate of post-acute symptoms, respectively.
Conclusions and relevance: These findings suggest that among previously immunologically naïve adults, few Omicron (BA.1/BA.2) and Delta infections are asymptomatic, and relative to Delta, Omicron infections were less likely to seek healthcare and experience post-acute symptoms.
Figures



References
-
- World Health Organization. World Health Organization, WHO R&D Blueprint COVID-19 new variants: Knowledge gaps and research. Accessed August 11, 2022. https://cdn.who.int/media/docs/default-source/blue-print/covid-19-new-va...
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous