

Initial experience with pulsed field ablation for atrial fibrillation
- PMID: 36426226
- PMCID: PMC9679623
- DOI: 10.3389/fcvm.2022.959186
Initial experience with pulsed field ablation for atrial fibrillation
Abstract
Introduction: Pulsed field ablation (PFA) was recently introduced for the treatment of symptomatic atrial fibrillation (AF) with the claim of selectively ablating the myocardium while sparing surrounding tissues. We present our initial experience with a PFA catheter for pulmonary vein isolation (PVI) and describe procedural findings and peri-procedural safety of the first 100 patients.
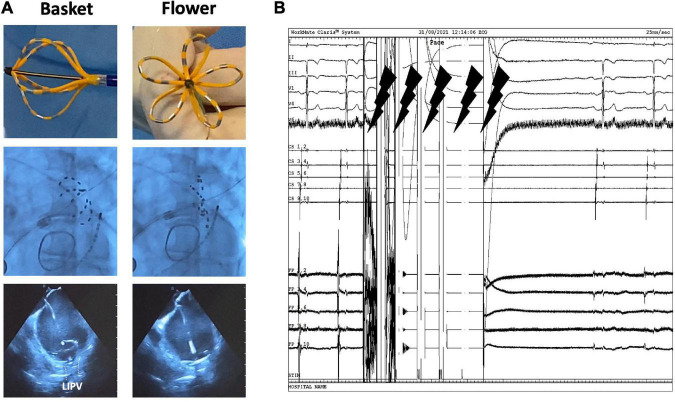
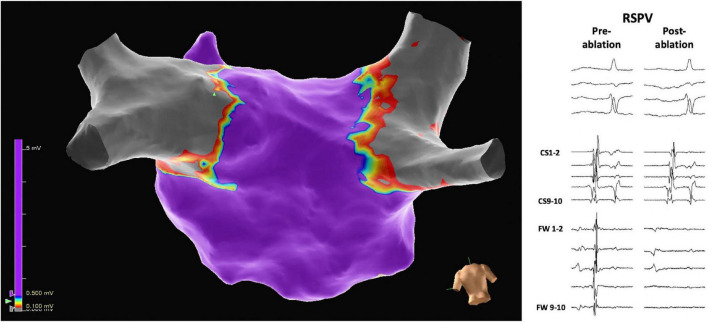
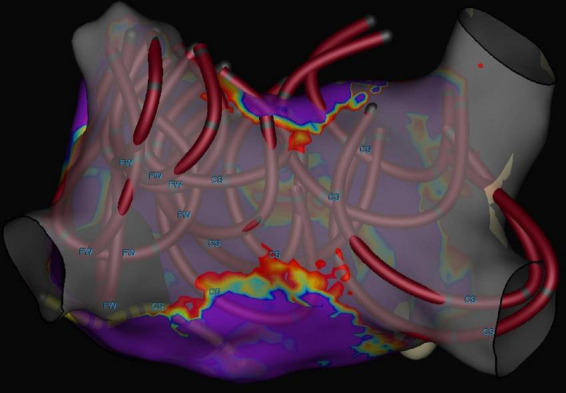
Materials and methods: We investigated 100 patients treated for symptomatic AF using the FARAWAVE PFA catheter (Farapulse, Menlo Park, CA, USA) between July 2021 and March 2022. Procedure workflow and electrophysiological findings at the time of ablation, peri-procedural complications, and operator learning curves are described.
Results: The mean age of patients was 62.9 ± 9.4 years, 62% were male subjects and 80% had paroxysmal AF. The median CHA2DS2-VASc score was 1.5 (IQR: 1.0-2.0) and the mean left atrial volume index was 35.7 ± 9.6 ml/m2. In 88 (88%) patients, PVI alone was performed and in 12 (12%) patients additional ablation of the posterior wall was performed. 3D-electroanatomic mapping was performed in 18 (18%) patients. Procedures without mapping lasted for 52.3 ± 16.6 min. The mean number of applications per pulmonary vein (PV) was 8.1 ± 0.6. In all patients (100%), all PVs were confirmed to be isolated. The learning curves of the two operators who performed > 20 procedures showed a negligible variation of performance over time and practice did not significantly predict procedure time [Operator 1 (senior): R 2 = 0.034, p = 0.35; Operator 2 (junior): R 2 = 0.004, p = 0.73]. There was no difference between the procedure times between senior and junior operators (Operator 1: 46.9 ± 9.7 min vs. Operator 2: 45.9 ± 9.9 min; p = 0.73). The only complications observed were two cases of bleeding at the site of percutaneous access.
Conclusion: Our initial experience shows that use of the PFA catheter for pulmonary vein isolation (PVI) is safe, fast, and easy to learn.
Keywords: atrial fibrillation; catheter ablation; learning curve; posterior wall ablation; pulsed field ablation.
Copyright © 2022 Magni, Mulder, Groenveld, Wiesfeld, Tieleman, Cox, Van Gelder, Smilde, Tan, Rienstra and Blaauw.
Conflict of interest statement
Author HG received a speaker fee from Biosense Webster. Author YB received research grants (to department) from AtriCure and Medtronic, and a speaker fee from AtriCure and Circle. He was also a proctor for Abbott, Biosense Webster, and Boston Scientific. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Hindricks G, Potpara T, Dagres N, Bax JJ, Boriani G, Dan GA, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eu Heart J. (2021) 42:373–498. - PubMed
-
- Ciconte G, Velagić V, Mugnai G, Saitoh Y, Irfan G, Hunuk B, et al. Electrophysiological findings following pulmonary vein isolation using radiofrequency catheter guided by contact-force and second-generation cryoballoon: lessons from repeat ablation procedures. Europace. (2015) 18:71–7. 10.1093/europace/euv224 - DOI - PubMed
-
- Aryana A, Singh SM, Mugnai G, de Asmundis C, Kowalski M, Pujara DK, et al. Pulmonary vein reconnection following catheter ablation of atrial fibrillation using the second-generation cryoballoon versus open-irrigated radiofrequency: results of a multicenter analysis. J Interv Card Electrophysiol. (2016) 47:341–8. 10.1007/s10840-016-0172-z - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials