

Mild Encephalopathy/Encephalitis With a Reversible Splenial Lesion (MERS) and Longitudinally Extensive Transverse Myelitis (LETM) in Influenza B: Neurotropic Mechanisms and Diagnostic Challenges
- PMID: 36426329
- PMCID: PMC9681700
- DOI: 10.7759/cureus.30681
Mild Encephalopathy/Encephalitis With a Reversible Splenial Lesion (MERS) and Longitudinally Extensive Transverse Myelitis (LETM) in Influenza B: Neurotropic Mechanisms and Diagnostic Challenges
Abstract
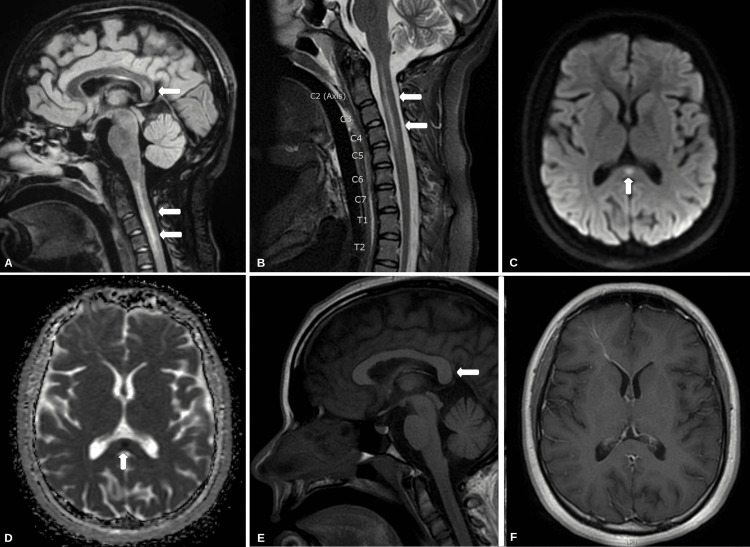
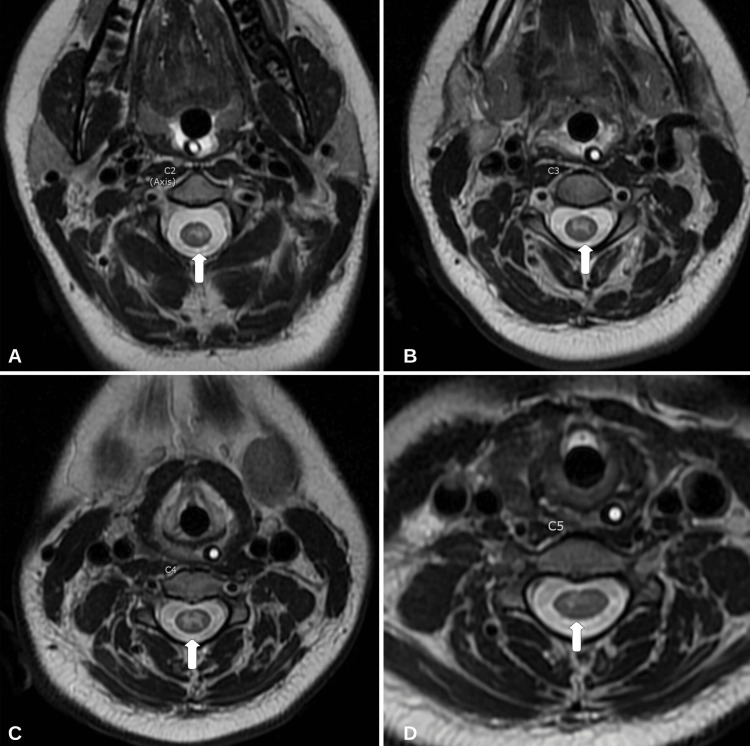
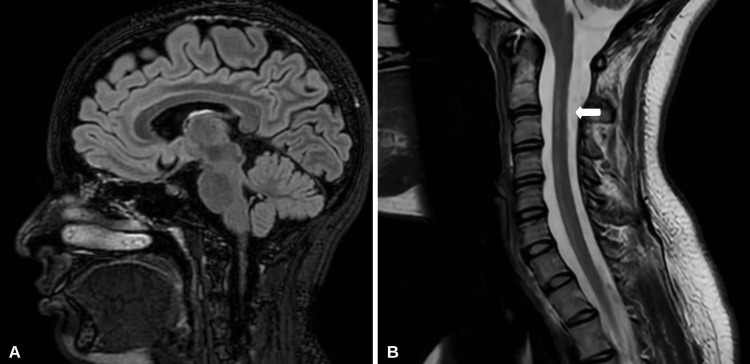
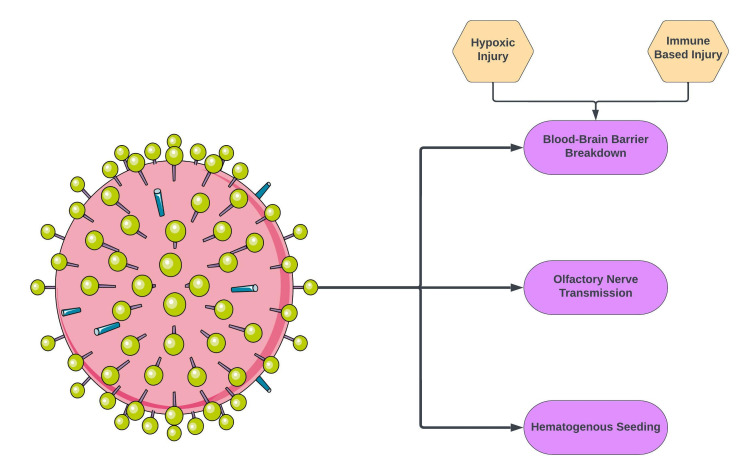
Mild encephalopathy/encephalitis with a reversible splenial lesion (MERS) and longitudinally extensive transverse myelitis (LETM) are neuroinflammatory conditions related to the brain and spinal cord, respectively. Most cases of MERS and LETM are related to a secondary autoimmune process in response to an initial insult (i.e., infection, immunization, etc.). The case of an 18-year-old female who developed a three-day history of fever, quadriplegia, cough, and mild encephalopathy is reported here. The patient tested positive for influenza B by nasopharyngeal swab with polymerase chain reaction (PCR). Initial magnetic resonance imaging (MRI) revealed the presence of a diffusion-restricted non-enhancing lesion confined to the splenium of the corpus callosum (MERS type I) and longitudinally extensive non-enhancing T2 hyperintensities from C1 to C5. The patient was managed with a five-day course of 1,000 mg of intravenous methylprednisolone (IVMP). Additionally, five days of therapeutic plasmapheresis (PLEX) was completed. The patient showed significant improvement with medical management and physical therapy. At the one-year follow-up, her motor symptoms had resolved and endorsed only mild paresthesia in the upper extremities. A repeat MRI revealed a reversal of the splenium lesion and moderate improvement in T2 hyperintensities of the cervical cord. Assessing neuroinvasion of the influenza virus is difficult, and diagnostic challenges arise in determining primary infectious versus autoimmune-mediated neuroinflammation. A review of the literature on influenza infection with radiographic findings of MERS and LETM is included.
Keywords: corpus callosum; encephalomyelitis; infectious encephalitis; influenza b; influenza virus; longitudinally extensive transverse myelitis; mild encephalopathy/encephalitis with reversible splenial lesion; neuroinfectious diseases; neurotropism; splenium.
Copyright © 2022, Srichawla et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Mild encephalitis/encephalopathy with a reversible splenial lesion associated with systemic Mycoplasma pneumoniae infection in North America: a case report.J Med Case Rep. 2022 Feb 20;16(1):74. doi: 10.1186/s13256-022-03299-6. J Med Case Rep. 2022. PMID: 35183255 Free PMC article.
-
Seropositive Neuromyelitis Optica in a Case of Undiagnosed Ankylosing Spondylitis: A Neuro-Rheumatological Conundrum.Qatar Med J. 2022 Jul 7;2022(3):29. doi: 10.5339/qmj.2022.29. eCollection 2022. Qatar Med J. 2022. PMID: 35864917 Free PMC article.
-
Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion in an Adult Patient with Influenza.Intern Med. 2017 Nov 15;56(22):3093-3095. doi: 10.2169/internalmedicine.8997-17. Epub 2017 Sep 25. Intern Med. 2017. PMID: 28943565 Free PMC article.
-
Mild encephalitis/encephalopathy with a reversible splenial lesion secondary to encephalitis complicated by hyponatremia: A case report and literature review.Medicine (Baltimore). 2019 Nov;98(47):e17982. doi: 10.1097/MD.0000000000017982. Medicine (Baltimore). 2019. PMID: 31764808 Free PMC article. Review.
-
Transient blindness associated with mild encephalitis/encephalopathy with a reversible splenial lesion (MERS): a case report and review of literature.Ital J Pediatr. 2020 Oct 12;46(1):152. doi: 10.1186/s13052-020-00918-0. Ital J Pediatr. 2020. PMID: 33046117 Free PMC article. Review.
Cited by
-
Polyarteritis Nodosa Following mRNA-1273 COVID-19 Vaccination: Case Study and Review of Immunological Mechanisms.Cureus. 2023 Jan 10;15(1):e33620. doi: 10.7759/cureus.33620. eCollection 2023 Jan. Cureus. 2023. PMID: 36788908 Free PMC article.
-
Influenza B-induced longitudinally extensive transverse myelitis and bithalamic acute disseminated encephalomyelitis.Neurol Sci. 2024 Mar;45(3):1299-1301. doi: 10.1007/s10072-023-07127-7. Epub 2023 Oct 17. Neurol Sci. 2024. PMID: 37848777
References
-
- Myelitis and other autoimmune myelopathies. Lopez Chiriboga S, Flanagan EP. Continuum (Minneap Minn) 2021;27:62–92. - PubMed
-
- Mild encephalitis/encephalopathy with reversible splenial lesion: a little-known entity with favourable prognosis. Gómez Iglesias P, López Valdés E, Vega Bayoll M, Gómez Ruíz MN. Neurologia (Engl Ed) 2020;35:581–583. - PubMed
-
- Mild encephalitis/encephalopathy with a reversible splenial lesion: five cases and a literature review. Pan JJ, Zhao YY, Lu C, Hu YH, Yang Y. Neurol Sci. 2015;36:2043–2051. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous