

Probiotics modulate gastrointestinal microbiota after Helicobacter pylori eradication: A multicenter randomized double-blind placebo-controlled trial
- PMID: 36426355
- PMCID: PMC9679295
- DOI: 10.3389/fimmu.2022.1033063
Probiotics modulate gastrointestinal microbiota after Helicobacter pylori eradication: A multicenter randomized double-blind placebo-controlled trial
Abstract
Background: Helicobacter pylori (H. pylori) eradication has been reported to cause short-term disruption of gut microbiota. It is acknowledged that probiotics supplementation mitigates side effects induced by H. pylori eradication, yet its role on alleviating dysbiosis of microbiota is obscure.
Objectives: To evaluate the impact of probiotics on gastrointestinal microbiota after eradication therapy.
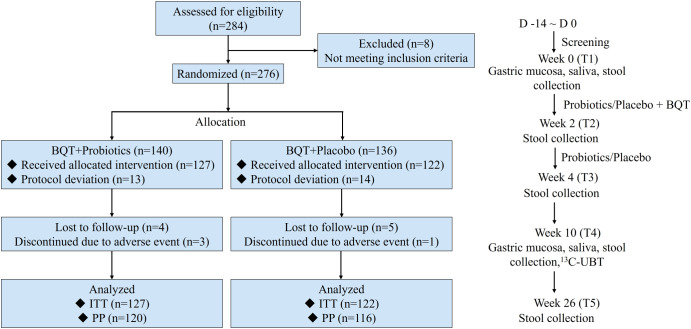
Methods: This was a multicenter, double-blinded, randomized trial done at seven centers in China. A total of 276 treatment-naïve H. pylori-positive patients were randomly assigned to receive 14-day bismuth-containing quadruple therapy (esomeprazole, bismuth, amoxicillin, furazolidone) combined with probiotics (Bifidobacterium Tetragenous viable Bacteria Tablets) (n=140) or placebo (n=136) for 28 days. Saliva, gastric mucosa and fecal samples were collected before and after therapy for 16S rRNA gene sequencing.
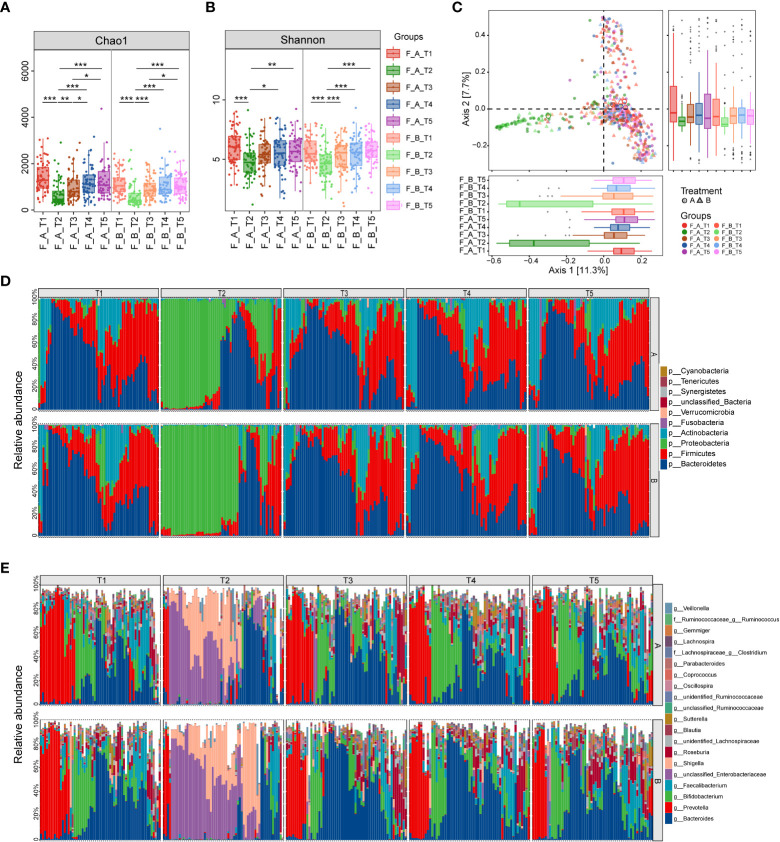
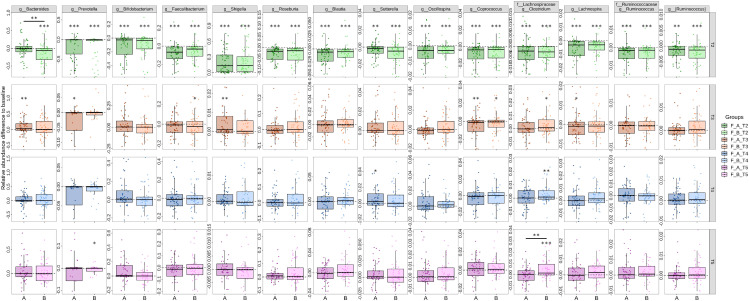
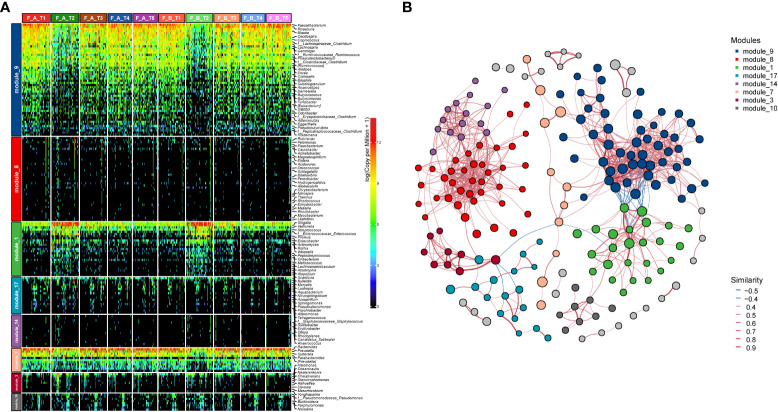
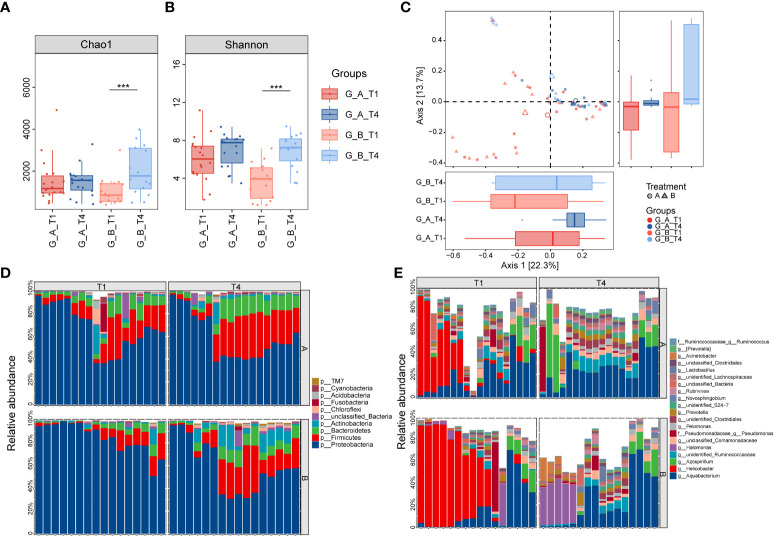
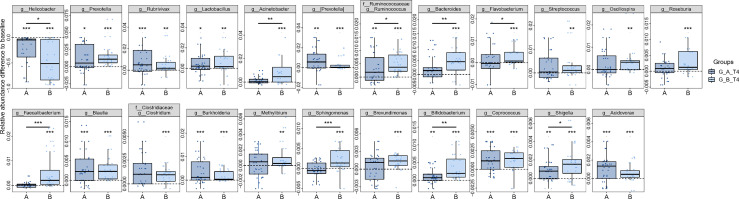
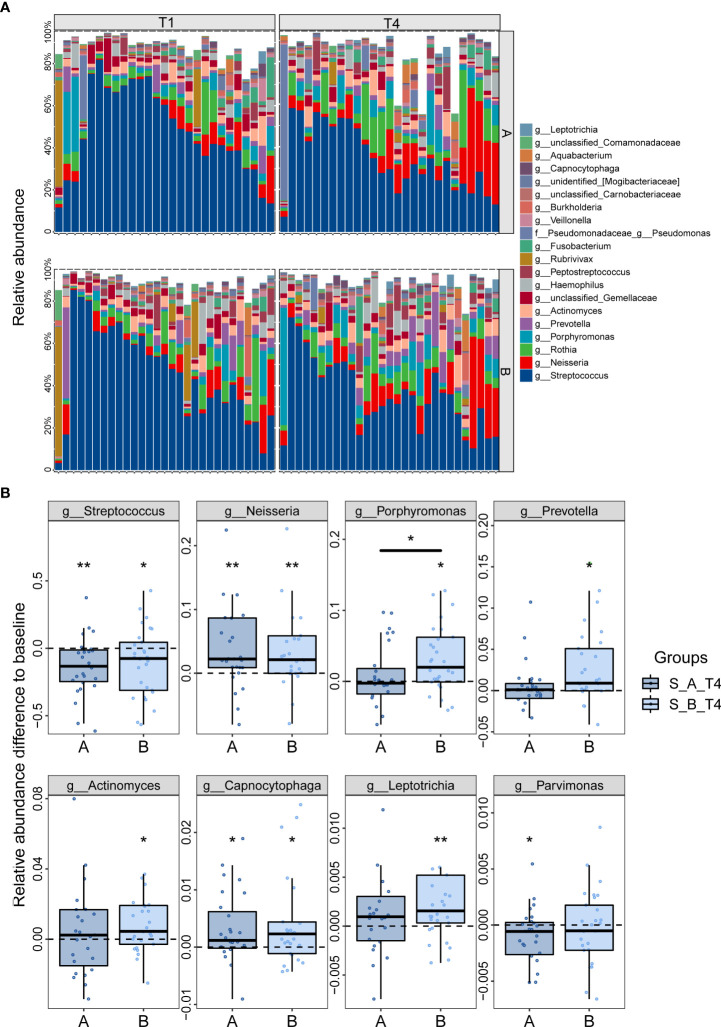
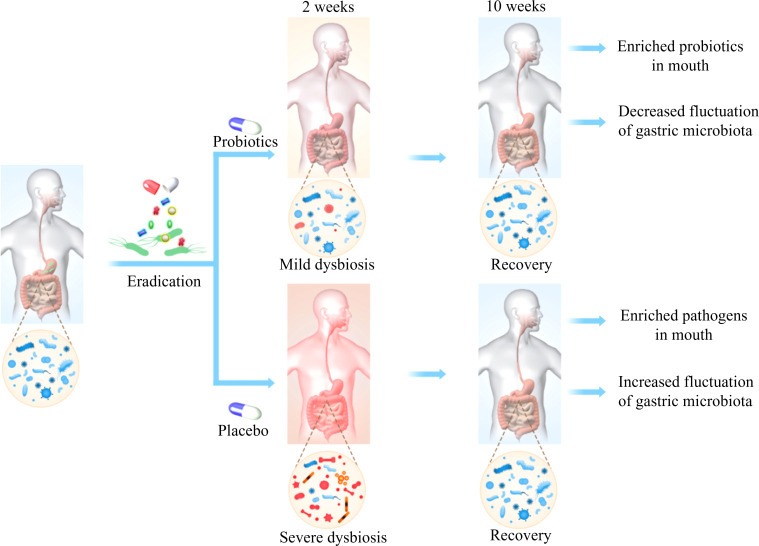
Results: The incidence of gastrointestinal adverse events was lower in probiotics group compared to placebo group (23.6% vs 37.7%, p=0.016), while there was no significant difference in eradication rate. We found dramatic perturbations of gut microbiota immediately following eradication, with the predominance of Proteobacteria in replacement of commensal Firmicutes and Bacteroidetes, and gradually restored after two weeks. The reduction of gut Bacteroidetes caused by eradication drugs was neutralized with probiotics supplementation. The gastric microbiota was completely reconstituted with H. pylori depleted and other taxa flourished. Of note, patients treated with probiotics showed smaller fluctuations of gastric microbiota compared to those with placebo. We also observed changes of saliva microbiota after H. pylori eradication, illustrated by the overgrowth of Neisseria and depletion of Streptococcus. The expansion of some pathogenic genera, including Porphyromonas, Leptotrichia, in the mouth was suppressed by probiotics.
Conclusion: This study not only demonstrated the beneficial effect of probiotics implementation on side events during H. pylori eradication but also provided a comprehensive profile of microbiome alterations along gastrointestinal tract that modulated by probiotics.
Keywords: 16S rRNA gene sequence; gastric microbiota; gut microbiota; helicobacter pylori eradication; probiotics; saliva microbiota.
Copyright © 2022 He, Xie, Zhu, Zhuang, Huo, Yu, Guo, Shu, Xiong, Zhang, Lyu and Lu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effect of probiotic supplementation combined with bismuth-containing quadruple therapy on gut microbiota during Helicobacter pylori eradication: a randomized, double-blind, placebo-controlled trial.Front Nutr. 2024 Oct 16;11:1484646. doi: 10.3389/fnut.2024.1484646. eCollection 2024. Front Nutr. 2024. PMID: 39479190 Free PMC article.
-
Helicobacter pylori eradication with bismuth quadruple therapy leads to dysbiosis of gut microbiota with an increased relative abundance of Proteobacteria and decreased relative abundances of Bacteroidetes and Actinobacteria.Helicobacter. 2018 Aug;23(4):e12498. doi: 10.1111/hel.12498. Epub 2018 Jun 13. Helicobacter. 2018. PMID: 29897654
-
Long-term effects of fecal microbiota transplantation on gut microbiota after Helicobacter pylori eradication with bismuth quadruple therapy: A randomized controlled trial.Helicobacter. 2024 Jul-Aug;29(4):e13079. doi: 10.1111/hel.13079. Helicobacter. 2024. PMID: 38984661 Clinical Trial.
-
The impact of probiotics on gut microbiota in the eradication of Helicobacter pylori infection: a systematic review.Eur Rev Med Pharmacol Sci. 2023 Jul;27(14):6736-6743. doi: 10.26355/eurrev_202307_33144. Eur Rev Med Pharmacol Sci. 2023. PMID: 37522685
-
Effects of Helicobacter pylori Therapy on Gut Microbiota: A Systematic Review and Meta-Analysis.Dig Dis. 2024;42(1):102-112. doi: 10.1159/000527047. Epub 2022 Oct 13. Dig Dis. 2024. PMID: 36228588
Cited by
-
Asia-Pacific Survey on the Management of Helicobacter pylori Infection.J Gastroenterol Hepatol. 2025 Apr;40(4):832-843. doi: 10.1111/jgh.16862. Epub 2024 Dec 26. J Gastroenterol Hepatol. 2025. PMID: 39726163 Free PMC article.
-
Impact of supplementing Limosilactobacillus fermentum MN-LF23 on the eradication of Helicobacter pylori with 14-day standard quadruple therapy: a randomized, double-blind, placebo-controlled trial.Nutr J. 2025 Jul 7;24(1):106. doi: 10.1186/s12937-025-01124-6. Nutr J. 2025. PMID: 40624535 Free PMC article. Clinical Trial.
-
Probiotics and Diet Modifications: A Holistic Approach to Tackling Helicobacter pylori with the Help of the Gut Microbiota.Probiotics Antimicrob Proteins. 2025 Aug 12. doi: 10.1007/s12602-025-10706-z. Online ahead of print. Probiotics Antimicrob Proteins. 2025. PMID: 40794147
-
Recent advances in therapeutic probiotics: insights from human trials.Clin Microbiol Rev. 2025 Jun 12;38(2):e0024024. doi: 10.1128/cmr.00240-24. Epub 2025 Apr 22. Clin Microbiol Rev. 2025. PMID: 40261032 Review.
-
Exploring the relationship between co-abundance of gut microbiota and novel metabolic pathways in different subtypes of irritable bowel syndrome: insights from the American Gut Project.Front Med (Lausanne). 2025 Jul 22;12:1615717. doi: 10.3389/fmed.2025.1615717. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40766067 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical