

Inflammatory conditions play a role in recurrence of PSC after liver transplantation: An international multicentre study
- PMID: 36426376
- PMCID: PMC9678780
- DOI: 10.1016/j.jhepr.2022.100599
Inflammatory conditions play a role in recurrence of PSC after liver transplantation: An international multicentre study
Abstract
Background & aims: Liver transplantation (LT) for primary sclerosing cholangitis (PSC) is complicated by recurrence of PSC (rPSC) in up to 25% of recipients. Recurrence has been shown to be detrimental for both graft and patient survival. For both PSC and rPSC, a medical cure is not available. To predict and ideally to prevent rPSC, it is imperative to find risk factors for rPSC that can be potentially modified. Therefore, we aimed to identify such factors for rPSC in a large international multicentre study including 6 centres in PSC-prevalent countries.
Methods: In this international multicentre, retrospective cohort study, 531 patients who underwent transplantation for PSC were included. In 25% of cases (n = 131), rPSC was diagnosed after a median follow-up of 6.72 (3.29-10.11) years post-LT.
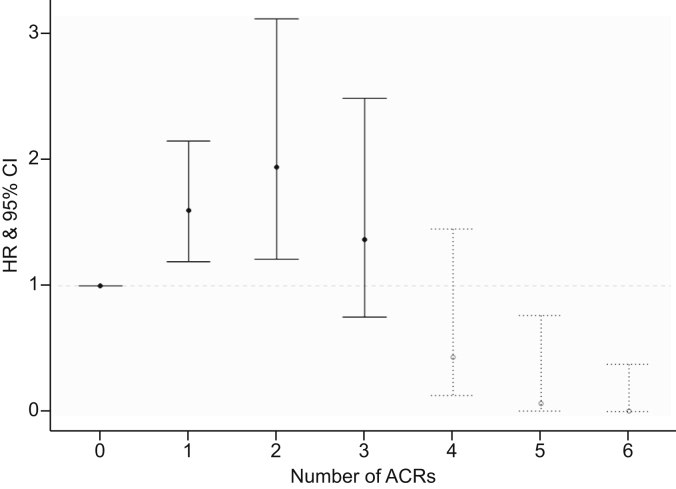
Results: In the multivariable competing risk model with time-dependent covariates, we found that factors representing an increased inflammatory state increase the risk for rPSC. Recurrent cholangitis before LT as indication for LT (hazard ratio [HR] 3.6, 95% CI 2.5-5.2), increased activity of inflammatory bowel disease after LT (HR 1.7, 95% CI 1.08-2.75), and multiple acute cellular rejections (HR: non-linear) were significantly and independently associated with an increased risk of rPSC. In contrast to the findings of previous studies, pretransplant colectomy was not found to be independently protective against the development of rPSC.
Conclusions: An increased inflammatory state before and after LT may play a causal and modifiable role in the development of rPSC. Pretransplant colectomy did not reduce the risk of rPSC per se. Recurrent cholangitis as indication for LT was associated with an increased risk of rPSC.
Impact and implications: Recurrence of PSC (rPSC) negatively affects survival after liver transplant (LT). Modifiable risk factors could guide clinical management and prevention of rPSC. We demonstrate that an increased inflammatory state both before and after LT increases the incidence of rPSC. As these are modifiable factors, they could serve as targets for future studies and therapies. We also added further evidence to the ongoing debate regarding preventive colectomy for rPSC by reporting that in our multicenter study, we could not find an independent association between colectomy and risk of rPSC.
Keywords: ACR, acute cellular rejection; CCA, cholangiocarcinoma; CD, Crohn's disease; Cholestatic liver disease; Colectomy; DBD, donation after brain death; DCD, donation after cardiac death; ELTR, European Liver Transplant Registry; HR, hazard ratio; IBD, inflammatory bowel disease; IBD-U, inflammatory bowel disease–unclassified; Inflammatory bowel disease; LD, living donor; LT, liver transplantation; Liver transplantation; MELD, model for end-stage liver disease; MRI, magnetic resonance imaging; PSC, primary sclerosing cholangitis; Primary sclerosing cholangitis; Recurrence of disease; Risk factors; SES-CD, Simple Endoscopic Score for Crohn's Disease; UC, ulcerative colitis; rPSC, recurrence of primary sclerosing cholangitis.
© 2022 The Author(s).
Conflict of interest statement
The authors who have taken part in this study declared that they do not have any conflict of interest with respect to this manuscript. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures




References
-
- Boonstra K., Weersma R.K., van Erpecum K.J., Rauws E.A., Spanier B.W., Poen A.C., et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology. 2013;58:2045–2055. - PubMed
-
- Lindkvist B., Benito de Valle M., Gullberg B., Björnsson E. Incidence and prevalence of primary sclerosing cholangitis in a defined adult population in Sweden. Hepatology. 2010;52:571–577. - PubMed
-
- Bambha K., Kim W.R., Talwalkar J., Torgerson H., Benson J.T., Therneau T.M., et al. Incidence, clinical spectrum, and outcomes of primary sclerosing cholangitis in a United States community. Gastroenterology. 2003;125:1364–1369. - PubMed
-
- Goet J.C., Hansen B.E., Tieleman M., van Hoek B., van den Berg A.P., Polak W.G., et al. Current policy for allocation of donor livers in The Netherlands advantages primary sclerosing cholangitis patients on the liver transplantation waiting list-a retrospective study. Transpl Int. 2018;31:590–599. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
