

Presentation, management, and outcomes of cauda equina syndrome up to one year after surgery, using clinician and participant reporting: A multi-centre prospective cohort study
- PMID: 36426378
- PMCID: PMC9678980
- DOI: 10.1016/j.lanepe.2022.100545
Presentation, management, and outcomes of cauda equina syndrome up to one year after surgery, using clinician and participant reporting: A multi-centre prospective cohort study
Abstract
Background: Cauda equina syndrome (CES) results from nerve root compression in the lumbosacral spine, usually due to a prolapsed intervertebral disc. Evidence for management of CES is limited by its infrequent occurrence and lack of standardised clinical definitions and outcome measures.
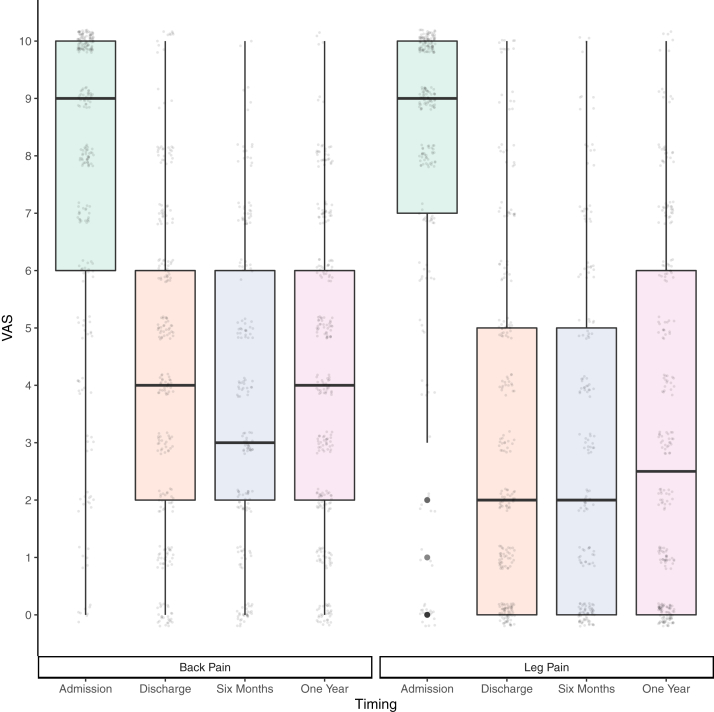
Methods: This is a prospective multi-centre observational cohort study of adults with CES in the UK. We assessed presentation, investigation, management, and all Core Outcome Set domains up to one year post-operatively using clinician and participant reporting. Univariable and multivariable associations with the Oswestry Disability Index (ODI) and urinary outcomes were investigated.
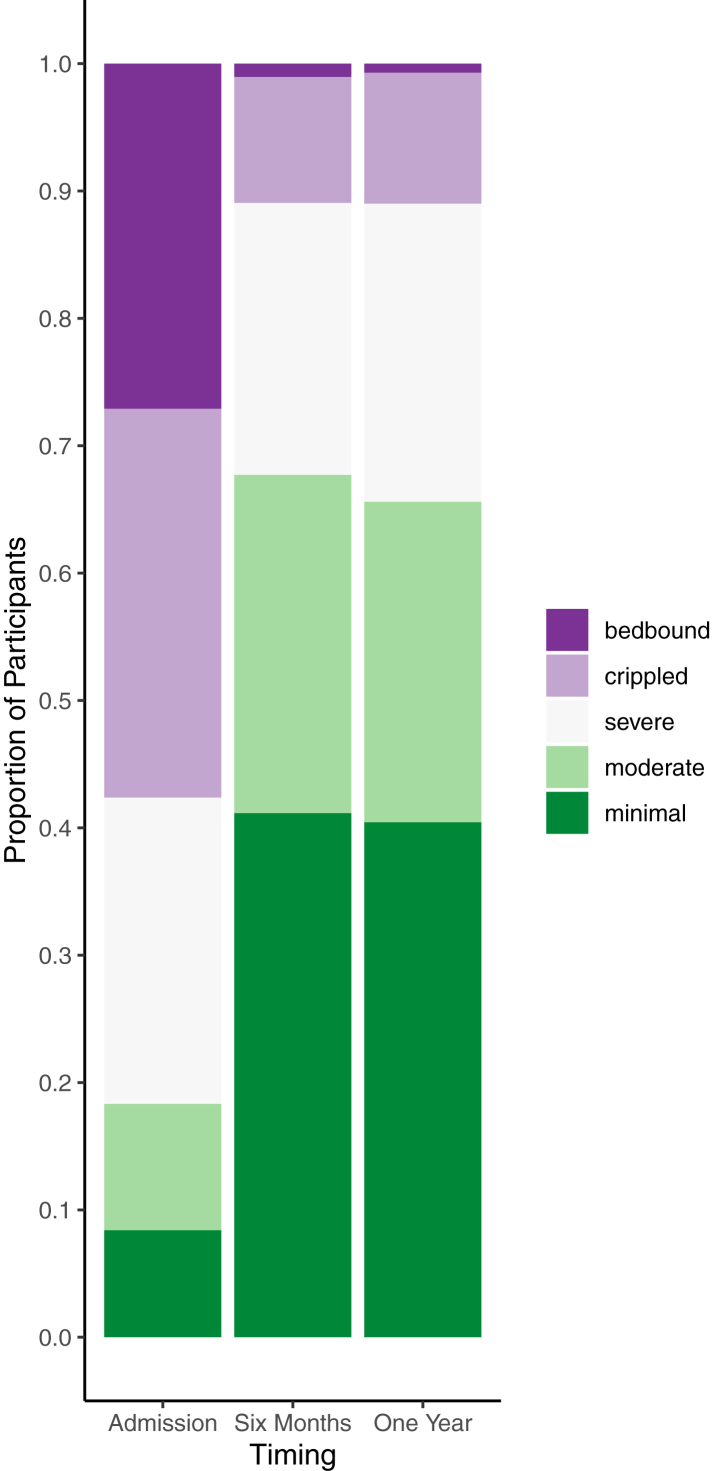
Findings: In 621 participants with CES, catheterisation for urinary retention was required pre-operatively in 31% (191/615). At discharge, only 13% (78/616) required a catheter. Median time to surgery from symptom onset was 3 days (IQR:1-8) with 32% (175/545) undergoing surgery within 48 h. Earlier surgery was associated with catheterisation (OR:2.2, 95%CI:1.5-3.3) but not with admission ODI or radiological compression. In multivariable analyses catheter requirement at discharge was associated with pre-operative catheterisation (OR:10.6, 95%CI:5.8-20.4) and one-year ODI was associated with presentation ODI (r = 0.3, 95%CI:0.2-0.4), but neither outcome was associated with time to surgery or radiological compression. Additional healthcare services were required by 65% (320/490) during one year follow up.
Interpretation: Post-operative functional improvement occurred even in those presenting with urinary retention. There was no association between outcomes and time to surgery in this observational study. Significant healthcare needs remained post-operatively.
Funding: DCN Endowment Fund funded study administration. Castor EDC provided database use. No other study funding was received.
Keywords: Back pain; Cauda equina syndrome; Cohort study; Spinal surgery; Urinary retention.
© 2022 The Authors.
Conflict of interest statement
JW, AABJ, JJ, SL, SP, CJH, AW, LH, RDCM, SD, HR, PCC, MTCP, NS, GG, NE, and PJS declare no conflicts of interest during the study or within 3 years of the work being submitted. IH declares support for attending meetings and payment or honoraria for speaking about functional neurological disorders (including persistent postural perceptual dizziness) at conferences and meetings. IH has received payment for expert testimony on idiopathic urinary retention. PFXS has received payment for expert testimony, acting for a number of both claimants and defenders in cases of Cauda Equina Syndrome, roughly in the proportion 2/3 defender, 1/3 claimant over about 20 years. PT has received payment for expert testimony for Cauda Equina Syndrome cases for DAC Beachcroft, Aspire Law, Bevan Brittan LLP, Stephensons LLP, Moore Barlow Ltd, Scott Rees & Co, and Premex/Premex +. AKD declares payment or honoraria for speaking for Integra, Stryker, and Safe Orthopaedics. AKD declares leadership board roles (unpaid) for Global Neuro Foundation and European Association of Neurosurgical Societies.
Figures



References
-
- Gleave J.R., Macfarlane R. Cauda equina syndrome: what is the relationship between timing of surgery and outcome? Br J Neurosurg. 2002;16(4):325–328. [published Online First: 2002/10/23] - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
