

Distinct Endotypes of Pediatric Rhinitis Based on Cluster Analysis
- PMID: 36426400
- PMCID: PMC9709680
- DOI: 10.4168/aair.2022.14.6.730
Distinct Endotypes of Pediatric Rhinitis Based on Cluster Analysis
Abstract
Purpose: Despite the wide spectrum of pediatric rhinitis, endotyping of rhinitis based on type 2 inflammation and bronchial hyper-responsiveness (BHR) is lacking. This study aimed to investigate endotypes of pediatric rhinitis using cluster analysis.
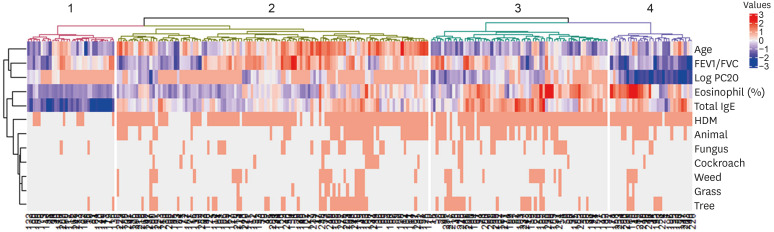
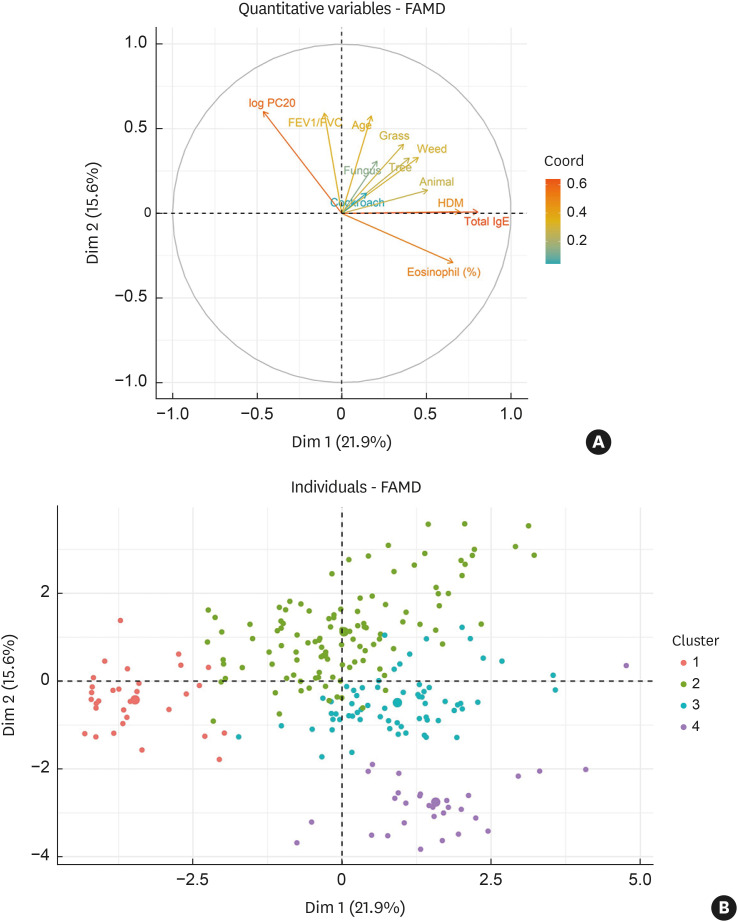
Methods: Cluster analysis was performed on data from 241 children with rhinitis by using 12 variables reflecting clinical characteristics of skin prick, laboratory, and pulmonary function tests. After extracting clusters, between-cluster differences in clinical features, such as nasal symptom scores and asthma comorbidity, were assessed to investigate the association between the endotypes and clinical features.
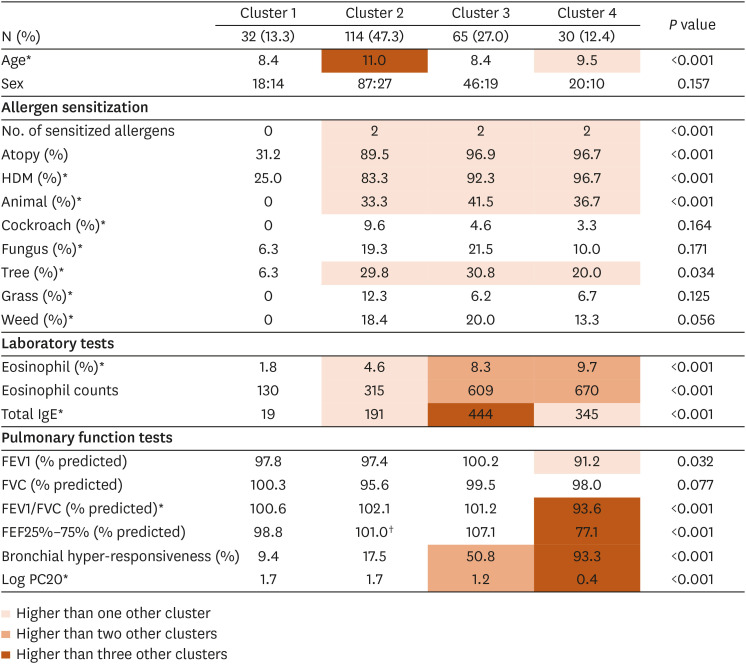
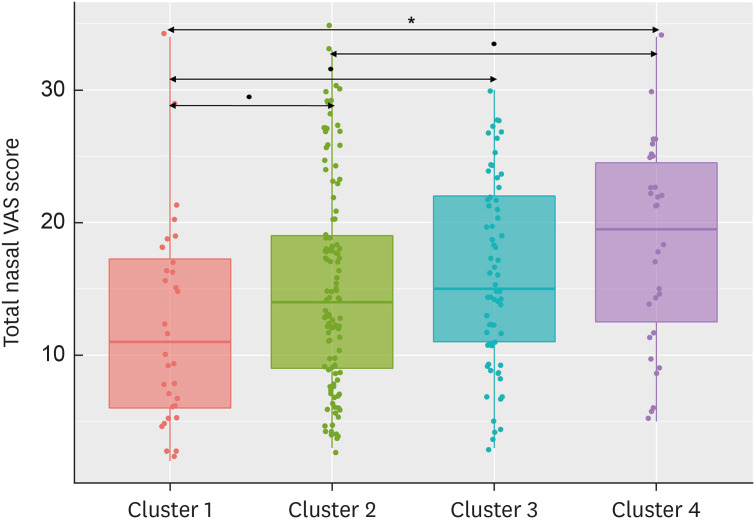
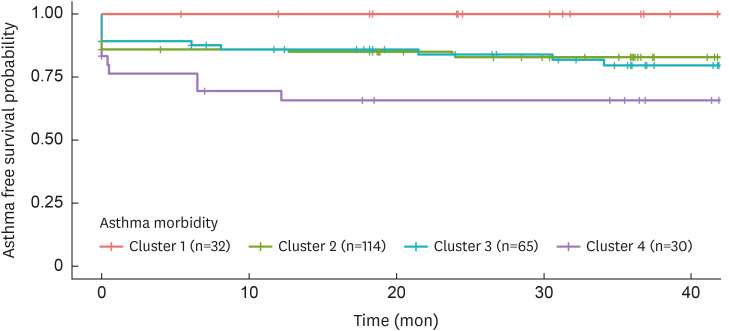
Results: Four clusters were extracted by hierarchical cluster analysis. Cluster 1 (n = 32 [13.3%]) was the non-allergic rhinitis dominant cluster with low type 2 inflammation and the lowest rate of BHR. Patients in cluster 1 had the mildest nasal symptoms and no asthma comorbidity. Cluster 2 (n = 114 [47.3%]) was the largest cluster and exhibited intermediate type 2 inflammation and low BHR. Cluster 3 (n = 65 [27.0%]) showed high type 2 inflammation and intermediate BHR. However, the severity of nasal symptoms and asthma comorbidity in this cluster were comparable with those in cluster 2. Cluster 4 (n = 30 [12.4%]) revealed high type 2 inflammation and BHR with potential functional airway impairment. Additionally, cluster 4 displayed the most severe nasal symptoms and frequent asthma comorbidity.
Conclusions: Four distinct endotypes of pediatric rhinitis based on allergen sensitization, type 2 inflammation, and BHR correlate to symptoms and asthma comorbidity. These endotypes may aid clinicians in understanding the wide spectrum of pediatric rhinitis.
Keywords: Allergic rhinitis; asthma; bronchial hyper-responsiveness; bronchial hyperreactivity; child; cluster analysis; pediatric rhinitis; rhinitis; type 2 inflammation.
Copyright © 2022 The Korean Academy of Asthma, Allergy and Clinical Immunology • The Korean Academy of Pediatric Allergy and Respiratory Disease.
Conflict of interest statement
There are no financial or other issues that might lead to conflict of interest.
Figures
Similar articles
-
Early bronchial airflow impairment in patients with persistent allergic rhinitis and bronchial hyperreactivity.Respir Med. 2005 Dec;99(12):1606-12. doi: 10.1016/j.rmed.2005.03.030. Epub 2005 Apr 26. Respir Med. 2005. PMID: 16291083
-
Upper and lower airway pathology in young children with allergic- and non-allergic rhinitis.Dan Med Bull. 2011 May;58(5):B4278. Dan Med Bull. 2011. PMID: 21535990 Review.
-
Relationship between nasal and bronchial responsiveness in perennial allergic rhinitic patients with asthma.Int Arch Allergy Immunol. 2002 Dec;129(4):341-7. doi: 10.1159/000067593. Int Arch Allergy Immunol. 2002. PMID: 12483039
-
Bronchial hyperresponsiveness in pediatric rhinitis patients: the difference between allergic and nonallergic rhinitis.Am J Rhinol Allergy. 2013 May-Jun;27(3):e63-8. doi: 10.2500/ajra.2013.27.3877. Am J Rhinol Allergy. 2013. PMID: 23710946
-
[Allergic rhinitis and bronchial hyperreactivity].Allergol Immunopathol (Madr). 2004 Nov-Dec;32(6):340-3. doi: 10.1016/s0301-0546(04)79266-6. Allergol Immunopathol (Madr). 2004. PMID: 15617661 Review. Spanish.
Cited by
-
Diagnosis and Management of Allergic Rhinitis in Asthmatic Children.J Asthma Allergy. 2023 Jan 5;16:45-57. doi: 10.2147/JAA.S281439. eCollection 2023. J Asthma Allergy. 2023. PMID: 36636703 Free PMC article. Review.
-
[Risk factors for the development of airway hyperresponsiveness in patients with allergic rhinitis].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023 Jun;37(6):457-462. doi: 10.13201/j.issn.2096-7993.2023.06.010. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023. PMID: 37253520 Free PMC article. Review. Chinese.
-
Clinical and molecular analysis of longitudinal rhinitis phenotypes in an urban birth cohort.J Allergy Clin Immunol. 2025 Feb;155(2):547-556. doi: 10.1016/j.jaci.2024.08.031. Epub 2024 Sep 20. J Allergy Clin Immunol. 2025. PMID: 39307288
-
Artificial intelligence in pediatric allergy research.Eur J Pediatr. 2024 Dec 21;184(1):98. doi: 10.1007/s00431-024-05925-5. Eur J Pediatr. 2024. PMID: 39706990 Free PMC article. Review.
-
Rhinoconjunctivitis symptoms in children and adolescents with asthma: Longitudinal clustering analysis.J Allergy Clin Immunol. 2025 May;155(5):1490-1498.e10. doi: 10.1016/j.jaci.2024.12.1084. Epub 2025 Jan 2. J Allergy Clin Immunol. 2025. PMID: 39755282
References
-
- de Benedictis FM, del Giudice MM, Jr, Severini S, Bonifazi F. Rhinitis, sinusitis and asthma: one linked airway disease. Paediatr Respir Rev. 2001;2:358–364. - PubMed
-
- Grossman J. One airway, one disease. Chest. 1997;111:11S–6S. - PubMed
-
- Rochat MK, Illi S, Ege MJ, Lau S, Keil T, Wahn U, et al. Allergic rhinitis as a predictor for wheezing onset in school-aged children. J Allergy Clin Immunol. 2010;126:1170–1175.e2. - PubMed
-
- van den Nieuwenhof L, Schermer T, Bosch Y, Bousquet J, Heijdra Y, Bor H, et al. Is physician-diagnosed allergic rhinitis a risk factor for the development of asthma? Allergy. 2010;65:1049–1055. - PubMed
-
- Bousquet J, Vignola AM, Demoly P. Links between rhinitis and asthma. Allergy. 2003;58:691–706. - PubMed
