

Present and future of the diagnostic work-up of multiple sclerosis: the imaging perspective
- PMID: 36427168
- PMCID: PMC9971159
- DOI: 10.1007/s00415-022-11488-y
Present and future of the diagnostic work-up of multiple sclerosis: the imaging perspective
Abstract
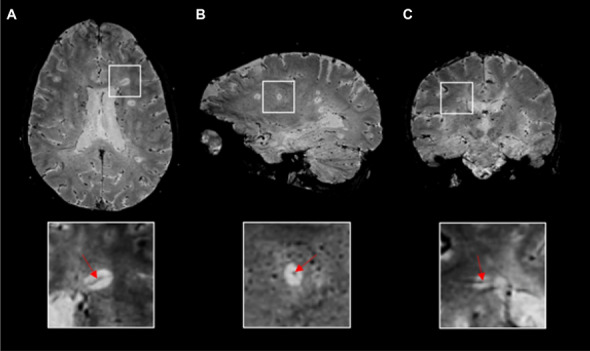
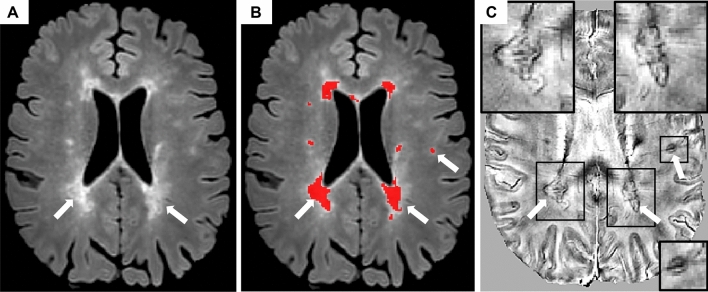
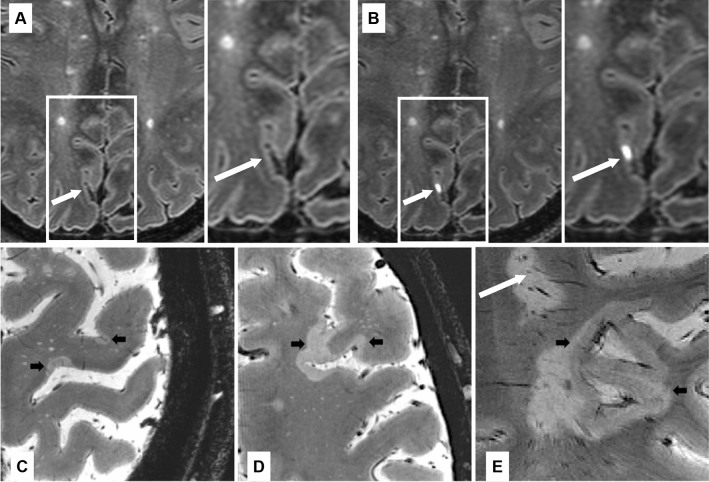
In recent years, the use of magnetic resonance imaging (MRI) for the diagnostic work-up of multiple sclerosis (MS) has evolved considerably. The 2017 McDonald criteria show high sensitivity and accuracy in predicting a second clinical attack in patients with a typical clinically isolated syndrome and allow an earlier diagnosis of MS. They have been validated, are evidence-based, simplify the clinical use of MRI criteria and improve MS patients' management. However, to limit the risk of misdiagnosis, they should be applied by expert clinicians only after the careful exclusion of alternative diagnoses. Recently, new MRI markers have been proposed to improve diagnostic specificity for MS and reduce the risk of misdiagnosis. The central vein sign and chronic active lesions (i.e., paramagnetic rim lesions) may increase the specificity of MS diagnostic criteria, but further effort is necessary to validate and standardize their assessment before implementing them in the clinical setting. The feasibility of subpial demyelination assessment and the clinical relevance of leptomeningeal enhancement evaluation in the diagnostic work-up of MS appear more limited. Artificial intelligence tools may capture MRI attributes that are beyond the human perception, and, in the future, artificial intelligence may complement human assessment to further ameliorate the diagnostic work-up and patients' classification. However, guidelines that ensure reliability, interpretability, and validity of findings obtained from artificial intelligence approaches are still needed to implement them in the clinical scenario. This review provides a summary of the most recent updates regarding the application of MRI for the diagnosis of MS.
Keywords: Diagnosis; Magnetic resonance imaging; Multiple sclerosis.
© 2022. The Author(s).
Conflict of interest statement
Massimo Filippi is Editor-in-Chief of the
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
