

Cancer Metastasis and Treatment Resistance: Mechanistic Insights and Therapeutic Targeting of Cancer Stem Cells and the Tumor Microenvironment
- PMID: 36428556
- PMCID: PMC9687343
- DOI: 10.3390/biomedicines10112988
Cancer Metastasis and Treatment Resistance: Mechanistic Insights and Therapeutic Targeting of Cancer Stem Cells and the Tumor Microenvironment
Abstract
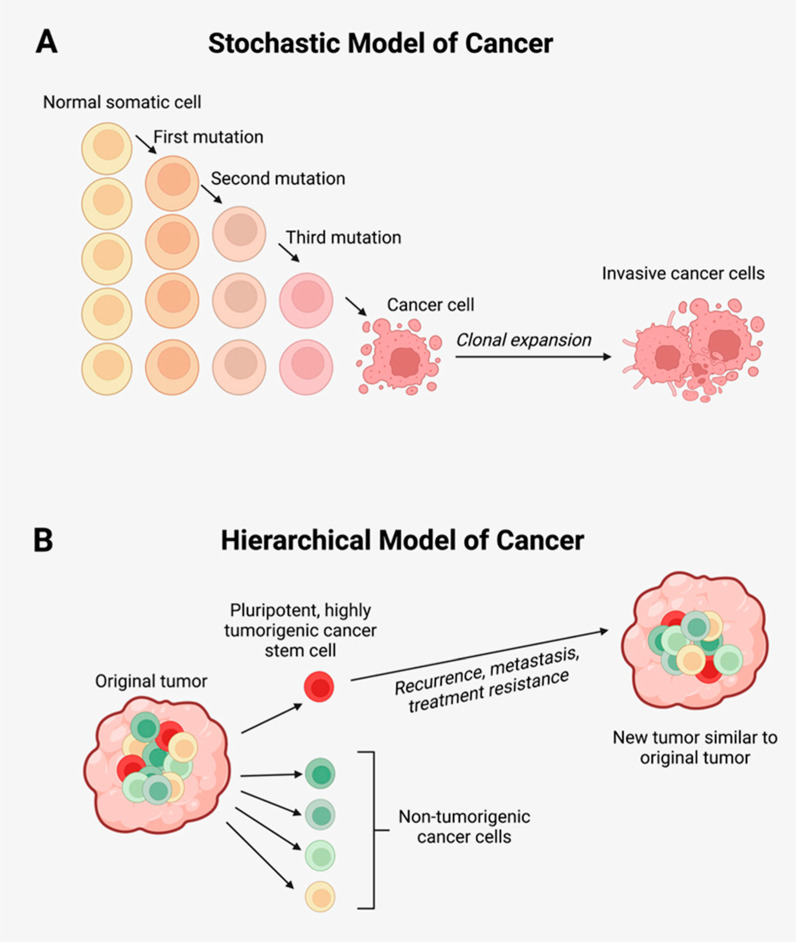
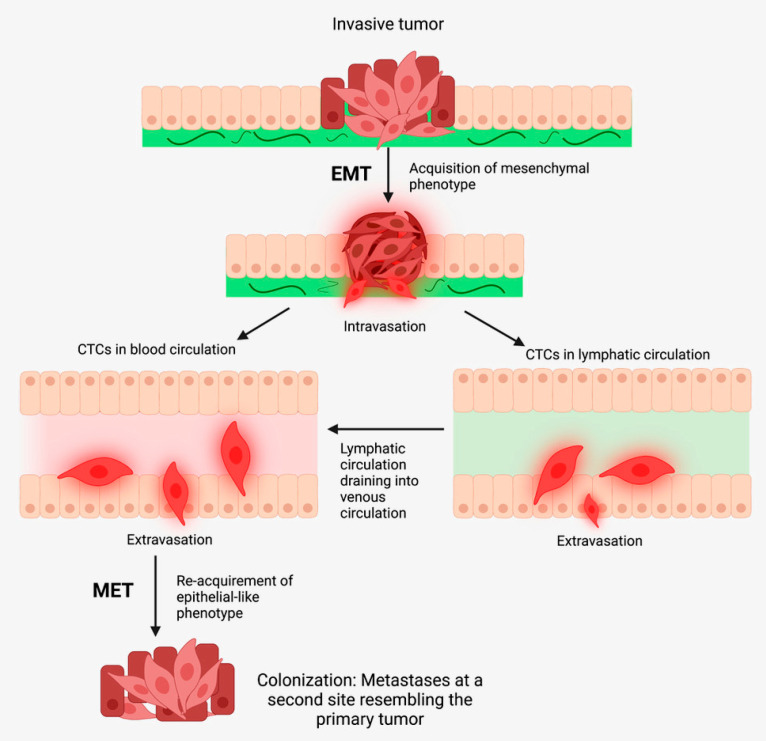
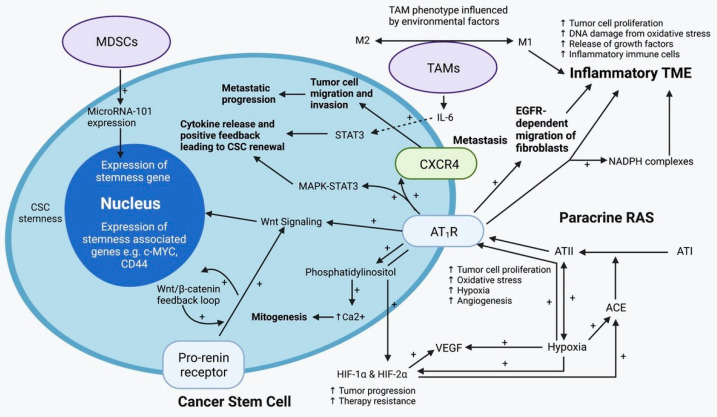
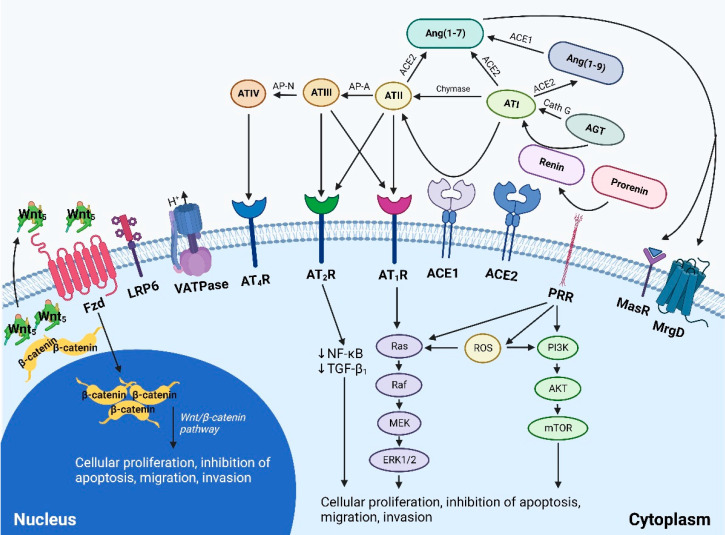
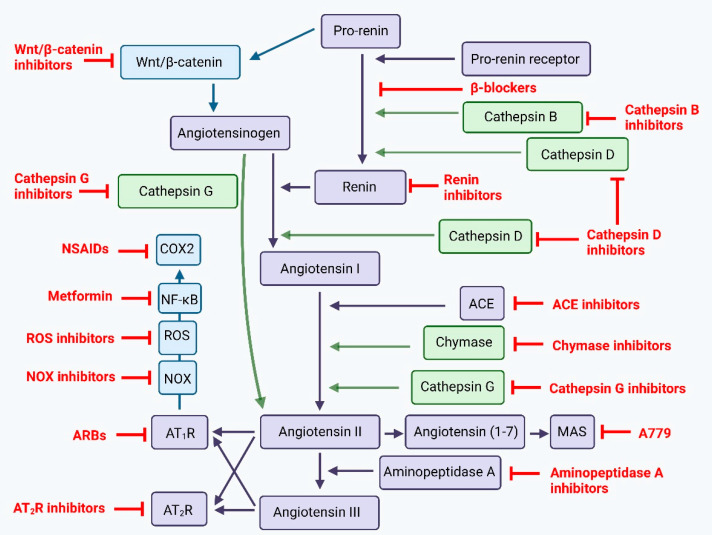
Cancer metastasis and treatment resistance are the main causes of treatment failure and cancer-related deaths. Their underlying mechanisms remain to be fully elucidated and have been attributed to the presence of cancer stem cells (CSCs)-a small population of highly tumorigenic cancer cells with pluripotency and self-renewal properties, at the apex of a cellular hierarchy. CSCs drive metastasis and treatment resistance and are sustained by a dynamic tumor microenvironment (TME). Numerous pathways mediate communication between CSCs and/or the surrounding TME. These include a paracrine renin-angiotensin system and its convergent signaling pathways, the immune system, and other signaling pathways including the Notch, Wnt/β-catenin, and Sonic Hedgehog pathways. Appreciation of the mechanisms underlying metastasis and treatment resistance, and the pathways that regulate CSCs and the TME, is essential for developing a durable treatment for cancer. Pre-clinical and clinical studies exploring single-point modulation of the pathways regulating CSCs and the surrounding TME, have yielded partial and sometimes negative results. This may be explained by the presence of uninhibited alternative signaling pathways. An effective treatment of cancer may require a multi-target strategy with multi-step inhibition of signaling pathways that regulate CSCs and the TME, in lieu of the long-standing pursuit of a 'silver-bullet' single-target approach.
Keywords: cancer stem cell; metastasis; renin-angiotensin system; treatment resistance; tumor microenvironment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
