

Features on Endoscopy and MRI after Treatment with Contact X-ray Brachytherapy for Rectal Cancer: Explorative Results
- PMID: 36428659
- PMCID: PMC9688812
- DOI: 10.3390/cancers14225565
Features on Endoscopy and MRI after Treatment with Contact X-ray Brachytherapy for Rectal Cancer: Explorative Results
Abstract
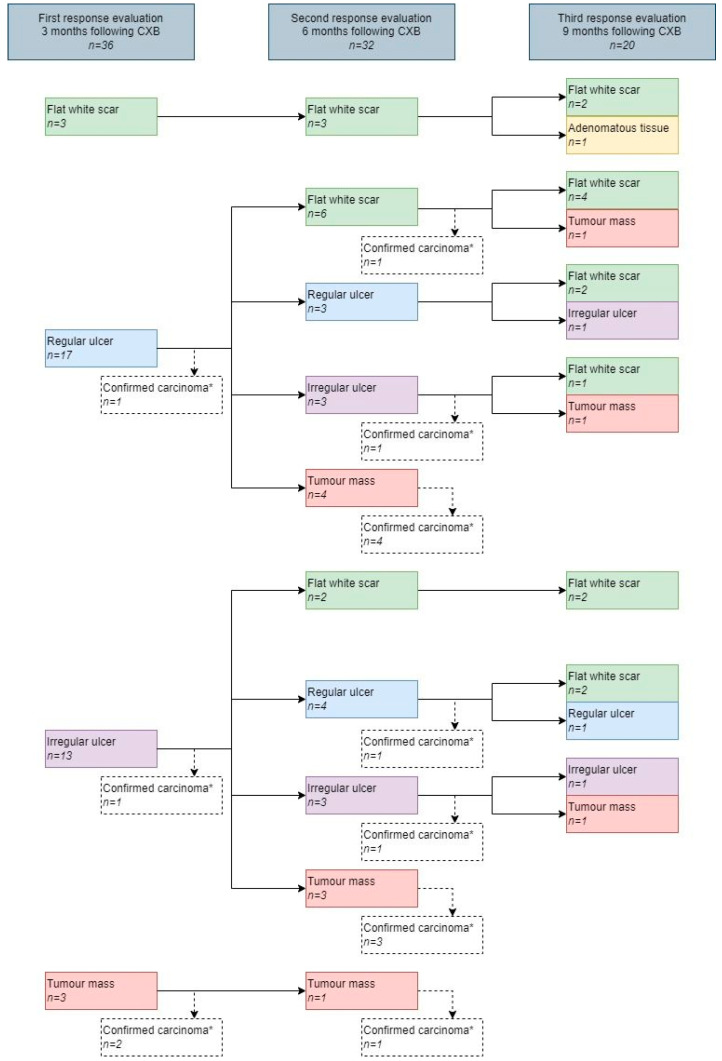
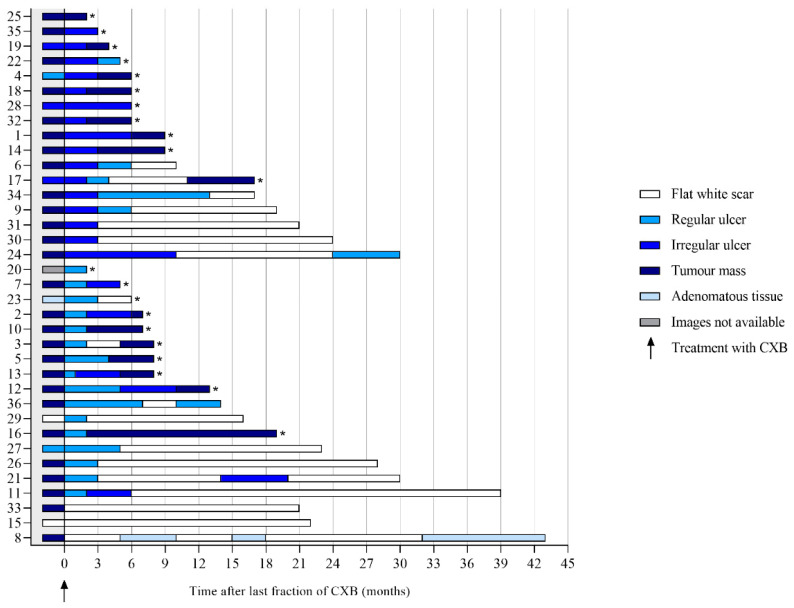
After neoadjuvant (chemo)radiotherapy for rectal cancer, contact X-ray brachytherapy (CXB) can be applied aiming at organ preservation. This explorative study describes the early features on endoscopy and MRI after CXB. Patients treated with CXB following (chemo)radiotherapy and a follow-up of ≥12 months were selected. Endoscopy and MRI were performed every 3 months. Expert readers scored all the images according to structured reporting templates. Thirty-six patients were included, 15 of whom obtained a cCR. On endoscopy, the most frequently observed feature early in follow-up was an ulcer, regardless of whether patients developed a cCR. A flat, white scar and tumor mass were common at 6 months. Focal tumor signal on T2W-MRI and mass-like high signal on DWI were generally absent in patients with a cCR. An ulceration on T2W-MRI and "reactive" mucosal signal on DWI were observed early in follow-up regardless of the final tumor response. The distinction between a cCR and a residual tumor generally can be made at 6 months. Features associated with a residual tumor are tumor mass on endoscopy, focal tumor signal on T2W-MRI, and mass-like high signal on DWI. Early recognition of these features is necessary to identify patients who will not develop a cCR as early as possible.
Keywords: MRI; contact X-ray brachytherapy; endoscopy; imaging; organ preservation; rectal cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Habr-Gama A., Perez R.O., Nadalin W., Sabbaga J., Ribeiro U., Jr., Silva e Sousa A.H., Jr., Campos F.G., Kiss D.R., Gama-Rodrigues J. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: Long-term results. Ann. Surg. 2004;240:711–717; discussion 717–718. doi: 10.1097/01.sla.0000141194.27992.32. - DOI - PMC - PubMed
-
- Maas M., Beets-Tan R.G., Lambregts D.M., Lammering G., Nelemans P.J., Engelen S.M., van Dam R.M., Jansen R.L., Sosef M., Leijtens J.W., et al. Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J. Clin. Oncol. 2011;29:4633–4640. doi: 10.1200/JCO.2011.37.7176. - DOI - PubMed
-
- Sun Myint A., Smith F.M., Gollins S., Wong H., Rao C., Whitmarsh K., Sripadam R., Rooney P., Hershman M., Pritchard D.M. Dose Escalation Using Contact X-ray Brachytherapy After External Beam Radiotherapy as Nonsurgical Treatment Option for Rectal Cancer: Outcomes From a Single-Center Experience. Int. J. Radiat. Oncol. Biol. Phys. 2018;100:565–573. doi: 10.1016/j.ijrobp.2017.10.022. - DOI - PubMed
LinkOut - more resources
Full Text Sources
