

Minimally Invasive Distal Pancreatectomy Techniques: A Contemporary Analysis Exploring Trends, Similarities, and Differences to Open Surgery
- PMID: 36428717
- PMCID: PMC9688336
- DOI: 10.3390/cancers14225625
Minimally Invasive Distal Pancreatectomy Techniques: A Contemporary Analysis Exploring Trends, Similarities, and Differences to Open Surgery
Abstract
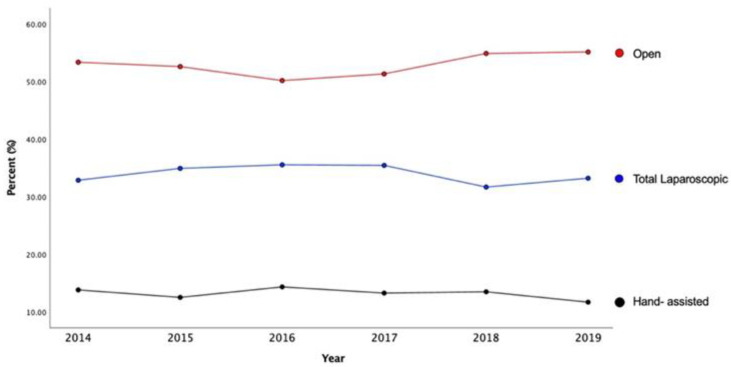
Limited contemporary data has compared similarities and differences between total laparoscopic (LDP), hand-assisted (HALDP), and open distal pancreatectomy (ODP). This study aimed to examine similarities and differences in outcomes between these three approaches in a contemporary cohort. Methods: Patients undergoing elective LDP, HALDP, and ODP in the NSQIP dataset (2014−2019) were included. Descriptive statistics and multivariate regression analyses were employed to compare postoperative outcomes. Results: Among 5636 patients, 33.9% underwent LDP, 13.1% HALDP, and 52.9% ODP. Compared with the LDP approach, surgical site infections were more frequent in HALDP and ODP approaches (1.2% vs. 2.6% vs. 2.8%, respectively, p < 0.01). After adjustment, the LDP approach was associated with a significantly lower likelihood of surgical site infection (OR 0.25, p = 0.03) when compared to ODP. There was no difference in the likelihood of surgical site infection when HALDP was compared to ODP (OR 0.59, p = 0.40). Unadjusted operative times were similar between approaches (LDP = 192 min, HALDP = 193 min, ODP = 191 min, p = 0.59). After adjustment, the LDP approach had a longer operative time (+10.3 min, p = 0.04) compared to ODP. There was no difference in the adjusted operative time between HALDP and ODP approaches (+5.4 min, p = 0.80). Conclusions: Compared to ODP, LDP was associated with improved surgical site infection rates and slightly longer operative times. There was no difference in surgical site infection rates between ODP and HALDP. Surgeon comfort and experience should decide the operative approach, but it is important to discuss the differences between these approaches with patients.
Keywords: distal pancreatectomy; hand-assisted laparoscopic; minimally invasive surgery; total laparoscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Venkat R., Edil B.H., Schulick R.D., Lidor A.O., Makary M.A., Wolfgang C.L. Laparoscopic distal pancreatectomy is associated with significantly less overall morbidity compared to the open technique: A systematic review and me-ta-analysis. Ann. Surg. 2012;255:1048–1059. doi: 10.1097/SLA.0b013e318251ee09. - DOI - PubMed
