

IETA Ultrasonic Features Combined with GI-RADS Classification System and Tumor Biomarkers for Surveillance of Endometrial Carcinoma: An Innovative Study
- PMID: 36428723
- PMCID: PMC9688181
- DOI: 10.3390/cancers14225631
IETA Ultrasonic Features Combined with GI-RADS Classification System and Tumor Biomarkers for Surveillance of Endometrial Carcinoma: An Innovative Study
Abstract
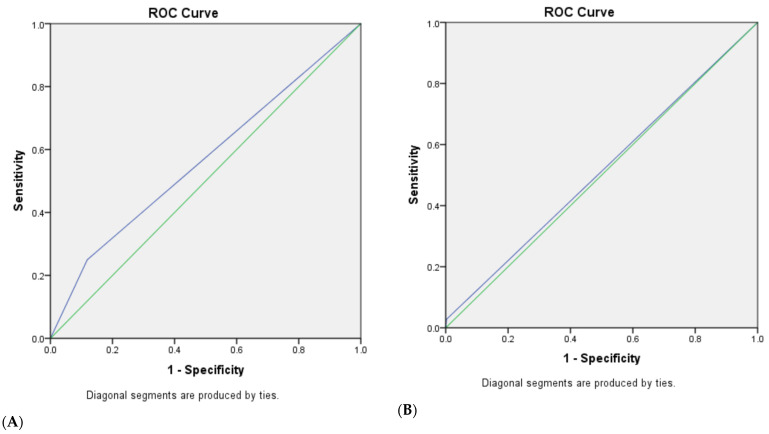
Objectives: We were the first to combine IETA ultrasonic features with GI-RADS and tumor biomarkers for the surveillance of endometrial carcinoma. The aim was to evaluate the efficacy of single IETA ultrasonography GI-RADS classification and combined tumor biomarkers in differentiating benign and malignant lesions in the uterine cavity and endometrium. Methods: A total of 497 patients with intrauterine and endometrial lesions who had been treated surgically between January 2017 and December 2021 were enrolled; all of them had undergone ultrasound examinations before surgery. We analyzed the correlation between the terms of ultrasonic signs of the uterine cavity and endometrial lesions defined by the expert consensus of IETA and the benign and malignant lesions and then classified these ultrasonic signs by GI-RADS. In addition, the tumor biomarkers CA125, CA15-3, CA19-9 and HE4 were combined by adjusting the classification. The results of the comprehensive analysis were compared with pathological results to analyze their diagnostic efficacy. Results: (1) The statistic analysis confirmed that there were seven independent predictors of malignant lesions, including thickened endometrium (premenopause ≥ 18.5 mm, postmenopause ≥ 15.5 mm), non-uniform endometrial echogenicity (heterogeneous with irregular cysts), endometrial midline appearance (not defined), the endometrial-myometrial junction (interrupted or not defined), intracavitary fluid (ground glass or "mixed" echogenicity), color score (3~4 points) and vascular pattern (focal origin multiple vessels or multifocal origin multiple vessels). (2) In traditional ultrasound GI-RADS (U-T-GI-RADS), if category 4a was taken as the cut-off value of benign and malignant, the diagnostic sensitivity, specificity, PPV, NPV and diagnostic accuracy were 97.2%, 65.2%, 44.0%, 98.8% and 72.2%, respectively, and the area under the ROC curve (AUC) was 0.812. If 4b was taken as the cut-off value, the diagnostic sensitivity, specificity, PPV, NPV diagnostic accuracy and AUC were 88.1%, 92.0%, 75.6%, 96.5% and 91.2%, 0.900, respectively. The diagnostic sensitivity, specificity, PPV, NPV diagnostic accuracy and AUC were 75.2%, 98.5%, 93.2%, 93.4%, 93.4% and 0.868, respectively, when taking category 5 as the cutoff point. In modified ultrasound GI-RADS (U-M-GI-RADS), if 4a was taken as the cut-off value, The diagnostic efficacy was the same as U-T-GI-RADS. If 4b was taken as the cut-off value, the diagnostic sensitivity, specificity, PPV, NPV, diagnostic accuracy and AUC were 88.1%, 92.3%, 76.2%, 96.5%, 91.3% and 0.902, respectively. If 4c was taken as the cutoff point, the diagnostic sensitivity, specificity, PPV, NPV diagnostic accuracy and AUC were 75.2%, 98.7%, 94.3%, 93.4%, 93.6% and 0.870, respectively. The diagnostic sensitivity, specificity, PPV, NPV diagnostic accuracy and AUC were 66.1%, 99.7%, 98.6%, 91.3%, 92.4% and 0.829, respectively, if taking category 5 as the cutoff point. (3) In the comprehensive diagnostic method of U-T-GI-RADS combined tumor biomarkers results, the AUC of class 4a, 4b and 5 as the cutoff value was 0.877, 0.888 and 0.738, respectively. The AUC of class 4a, 4b, 4c and 5 as the cutoff value in the comprehensive diagnostic method of U-M-GI-RADS combined tumor biomarkers results was 0.877, 0.888, 0.851 and 0.725, respectively. There was no significant difference in diagnostic efficiency between the two comprehensive diagnostic methods. Conclusions: In this study, no matter which diagnostic method was used, the best cutoff value for predicting malignant EC was ≥GI-RADS 4b. The GI-RADS classification had good performance in discriminating EC. The tumor biomarkers, CA125, CA19-9, CA15-3 and HE4, could improve the diagnostic efficacy for preoperative endometrial carcinoma assessment.
Keywords: endometrial cancer/carcinoma (EC); endometrium lesion; gynecologic imaging reporting and data system (GI-RADS); the international endometrial tumor analysis (IETA); tumor biomarkers; uterine cavity lesions.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Ge L., Liu G., Hu K., Huang K., Zhang M., Zhou J., Teng F., Cao J., Dai C., Jia X. A New Risk Index Combining d-Dimer, Fibrinogen, HE4, and CA199 Differentiates Suspecting Endometrial Cancer From Patients With Abnormal Vaginal Bleeding or Discharge. Technol. Cancer Res. Treat. 2020;19:1533033819901117. doi: 10.1177/1533033819901117. - DOI - PMC - PubMed
-
- Behrouzi R., Ryan N.A.J., Barr C.E., Derbyshire A.E., Wan Y.L., Maskell Z., Stocking K., Pemberton P.W., Bolton J., McVey R.J., et al. Baseline Serum HE4 But Not Tissue HE4 Expression Predicts Response to the Levonorgestrel-Releasing Intrauterine System in Atypical Hyperplasia and Early Stage Endometrial Cancer. Cancers. 2020;12:276. doi: 10.3390/cancers12020276. - DOI - PMC - PubMed
Grants and funding
- 82202262/National Natural Science Foundation of China
- 81972423/National Natural Science Foundation of China
- 2021A1515011585/the Province Natural Science Foundation of Guangdong
- JCYJ20190814110207603/General project of Science and Technology Innovation Committee of Shenzhen
- JCYJ20190814111801681/General project of Science and Technology Innovation Committee of Shenzhen
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
