

Contemporary Management of Postoperative Crohn's Disease after Ileocolonic Resection
- PMID: 36431223
- PMCID: PMC9693828
- DOI: 10.3390/jcm11226746
Contemporary Management of Postoperative Crohn's Disease after Ileocolonic Resection
Abstract
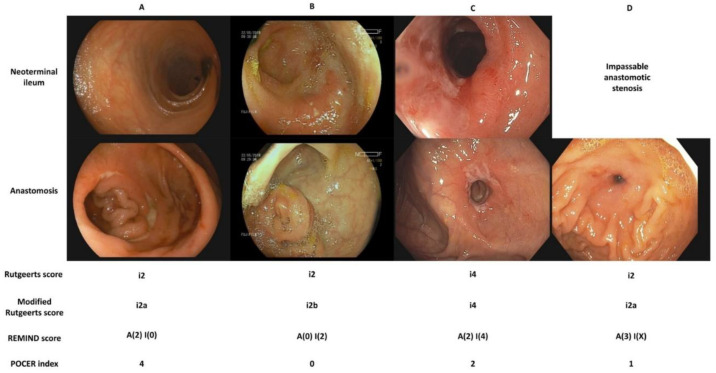
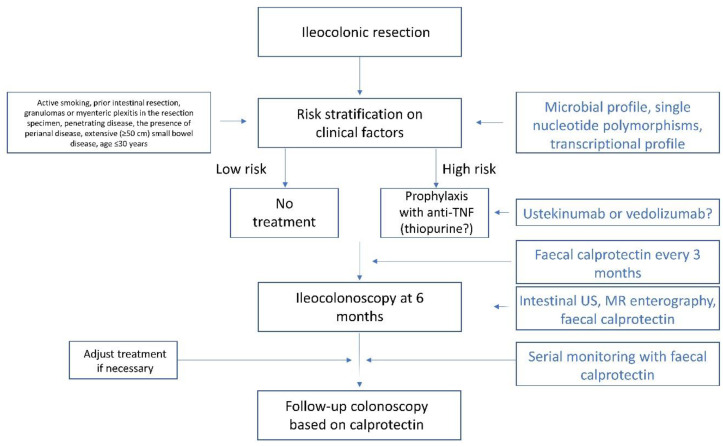
Surgery remains an important treatment modality in the multidisciplinary management of patients with Crohn's disease (CD). To illustrate the recent advances in the management of postoperative CD we outline the contemporary approach to treatment: diagnosing disease recurrence using endoscopy or noninvasive methods and risk stratification underlying decisions to institute treatment. Endoscopic scoring indices are being refined to guide treatment decisions by accurately estimating the risk of recurrence based on endoscopic appearance. The original Rutgeerts score has been modified to separate anastomotic lesions from lesions in the neoterminal ileum. Two further indices, the REMIND score and the POCER index, were recently developed with the same intention. Noninvasive monitoring for recurrence using a method with high negative predictive value has the potential to simplify management algorithms and only perform ileocolonoscopy in a subset of patients. Fecal calprotectin, intestinal ultrasound, and magnetic resonance enterography are all being evaluated for this purpose. The use of infliximab for the prevention of postoperative recurrence is well supported by data, but management decisions are fraught with uncertainty for patients with previous exposure to biologics. Data on the use of ustekinumab and vedolizumab for postoperative CD are emerging, but controlled studies are lacking.
Keywords: endoscopy; fecal calprotectin; intestinal ultrasound; magnetic resonance enterography; noninvasive monitoring; prophylaxis; surgery.
Conflict of interest statement
J.H.: speaker’s fees from Abbvie, Janssen, and Takeda; consulting fees from Alimentiv Inc. D.D. has served as a speaker, a consultant, and an advisory board member for Merck Sharp & Dohme, AbbVie, Takeda, Pfizer, Janssen, Amgen, Biogen, and Krka.
Figures
Similar articles
-
Differential risk of disease progression between isolated anastomotic ulcers and mild ileal recurrence after ileocolonic resection in patients with Crohn's disease.Gastrointest Endosc. 2019 Aug;90(2):269-275. doi: 10.1016/j.gie.2019.01.029. Epub 2019 Feb 6. Gastrointest Endosc. 2019. PMID: 30738034 Free PMC article.
-
A nomogram incorporating ileal and anastomotic lesions separately to predict the long-term outcome of Crohn's disease after ileocolonic resection.Therap Adv Gastroenterol. 2023 Sep 14;16:17562848231198933. doi: 10.1177/17562848231198933. eCollection 2023. Therap Adv Gastroenterol. 2023. PMID: 37720355 Free PMC article.
-
Adalimumab in prevention of postoperative recurrence of Crohn's disease in high-risk patients.World J Gastroenterol. 2012 Aug 28;18(32):4391-8. doi: 10.3748/wjg.v18.i32.4391. World J Gastroenterol. 2012. PMID: 22969204 Free PMC article.
-
Clinical Update on the Prevention and Management of Postoperative Crohn's Disease Recurrence.Curr Gastroenterol Rep. 2024 Feb;26(2):41-52. doi: 10.1007/s11894-023-00911-7. Epub 2024 Jan 16. Curr Gastroenterol Rep. 2024. PMID: 38227128 Review.
-
What's New in the Postoperative Management of Crohn's Disease?Dig Dis Sci. 2022 Aug;67(8):3508-3517. doi: 10.1007/s10620-021-07205-w. Epub 2021 Aug 18. Dig Dis Sci. 2022. PMID: 34406585 Free PMC article. Review.
Cited by
-
Preventing Recurrence of Crohn's Disease Post-Ileocaecal Surgery in Paediatric Patients: A Therapy Guide Based on Systematic Review of the Evidence.Paediatr Drugs. 2024 Nov;26(6):659-672. doi: 10.1007/s40272-024-00650-w. Epub 2024 Aug 31. Paediatr Drugs. 2024. PMID: 39215954
-
Comparing adalimumab and infliximab in the prevention of postoperative recurrence of Crohn's disease: a systematic review and meta-analysis.Ann Gastroenterol. 2023 May-Jun;36(3):293-299. doi: 10.20524/aog.2023.0786. Epub 2023 Apr 3. Ann Gastroenterol. 2023. PMID: 37144019 Free PMC article.
References
-
- Tsai L., Ma C., Dulai P.S., Prokop L.J., Eisenstein S., Ramamoorthy S.L., Feagan B.G., Jairath V., Sandborn W.J., Singh S. Contemporary Risk of Surgery in Patients With Ulcerative Colitis and Crohn’s Disease: A Meta-Analysis of Population-Based Cohorts. Clin. Gastroenterol. Hepatol. 2020;19:2031–2204. doi: 10.1016/j.cgh.2020.10.039. - DOI - PMC - PubMed
-
- Ma C., Moran G.W., Benchimol E.I., Targownik L.E., Heitman S.J., Hubbard J.N., Seow C.H., Novak K.L., Ghosh S., Panaccione R., et al. Surgical Rates for Crohn’s Disease are Decreasing: A Population-Based Time Trend Analysis and Validation Study. Am. J. Gastroenterol. 2017;112:1840–1848. doi: 10.1038/ajg.2017.394. - DOI - PMC - PubMed
-
- Frolkis A.D., Dykeman J., Negron M.E., Debruyn J., Jette N., Fiest K.M., Frolkis T., Barkema H.W., Rioux K.P., Panaccione R., et al. Risk of surgery for inflammatory bowel diseases has decreased over time: A systematic review and meta-analysis of population-based studies. Gastroenterology. 2013;145:996–1006. doi: 10.1053/j.gastro.2013.07.041. - DOI - PubMed
-
- Frolkis A.D., Lipton D.S., Fiest K.M., Negron M.E., Dykeman J., deBruyn J., Jette N., Frolkis T., Rezaie A., Seow C.H., et al. Cumulative incidence of second intestinal resection in Crohn’s disease: A systematic review and meta-analysis of population-based studies. Am. J. Gastroenterol. 2014;109:1739–1748. doi: 10.1038/ajg.2014.297. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
