

Anemia and Iron Deficiency in Outpatients with Inflammatory Bowel Disease: Ubiquitous Yet Suboptimally Managed
- PMID: 36431320
- PMCID: PMC9692778
- DOI: 10.3390/jcm11226843
Anemia and Iron Deficiency in Outpatients with Inflammatory Bowel Disease: Ubiquitous Yet Suboptimally Managed
Abstract
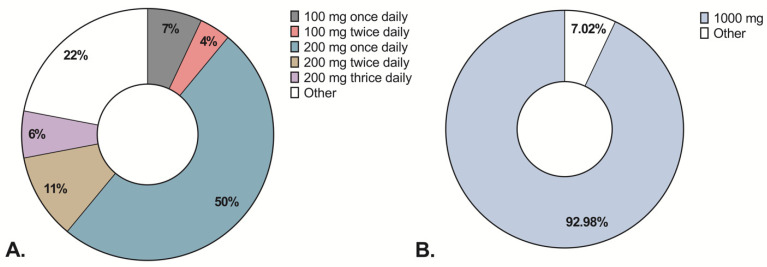
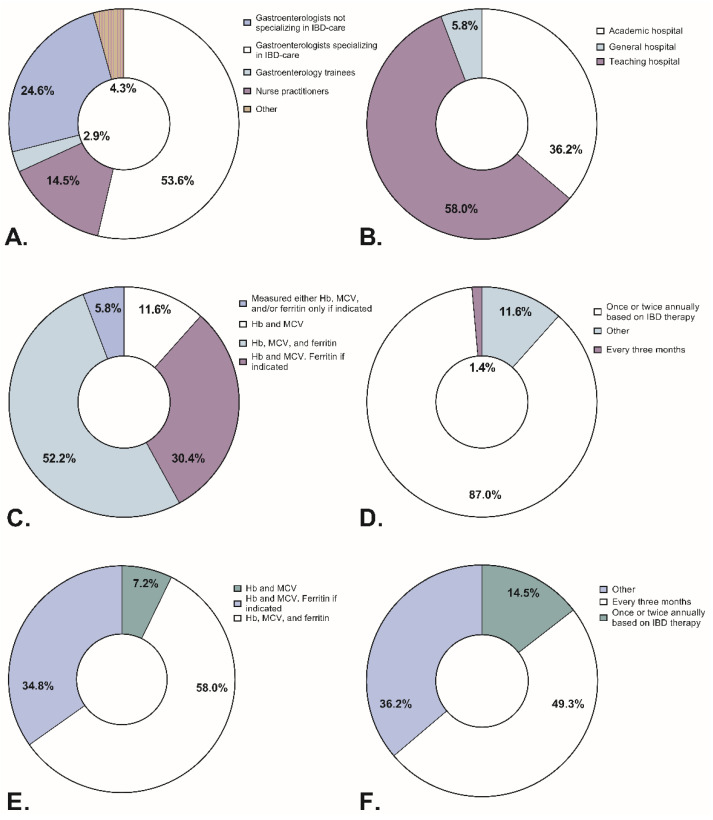
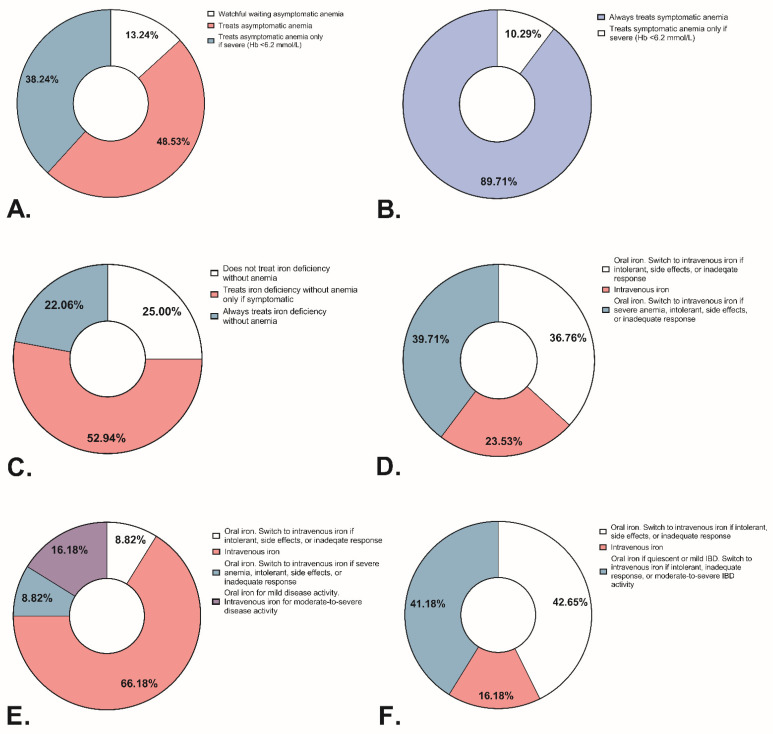
Background: Iron deficiency (ID) and anemia in patients with Inflammatory Bowel Disease (IBD) are associated with a reduced quality of life. We assessed the prevalence of ID and anemia in Dutch outpatients with IBD and compared routine ID(A) management among medical professionals to the European Crohn’s and Colitis Organisation (ECCO) treatment guidelines. Methods: Between January and November 2021, consecutive adult outpatients with IBD were included in this study across 16 Dutch hospitals. Clinical and biochemical data were extracted from medical records. Additionally, medical professionals filled out questionnaires regarding routine ID(A) management. Results: In total, 2197 patients (1271 Crohn’s Disease, 849 Ulcerative Colitis, and 77 IBD-unclassified) were included. Iron parameters were available in 59.3% of cases. The overall prevalence of anemia, ID, and IDA was: 18.0%, 43.4%, and 12.2%, respectively. The prevalence of all three conditions did not differ between IBD subtypes. ID(A) was observed more frequently in patients with biochemically active IBD than in quiescent IBD (ID: 70.8% versus 23.9%; p < 0.001). Contrary to the guidelines, most respondents prescribed standard doses of intravenous or oral iron regardless of biochemical parameters or inflammation. Lastly, 25% of respondents reported not treating non-anemic ID. Conclusions: One in five patients with IBD suffers from anemia that—despite inconsistently measured iron parameters—is primarily caused by ID. Most medical professionals treat IDA with oral iron or standard doses of intravenous iron regardless of biochemical inflammation; however, non-anemic ID is often overlooked. Raising awareness about the management of ID(A) is needed to optimize and personalize routine care.
Keywords: Inflammatory Bowel Disease; anemia; iron deficiency.
Conflict of interest statement
G.D. received research grants from Royal DSM and speaker’s fees from Janssen Pharmaceuticals, Takeda, Pfizer, and Abbvie. A.E.v.d.M.-d.J. received unrestricted research grants from Galapagos, Norgine, Vedanta and Nestle, including speaker’s fees from Galapagos, Tramedico, Takeda, and Janssen Pharmaceuticals. R.L. has received travel expenses and speaker’s fees from Cablon Medical. A.A.v.B. has received speaker’s fees and research grants from AbbVie, Arandal, Arena, Celgene, Ferring, Janssen, MSD, Pfizer, Roche, Takeda, TEVA, ZonMW and Eurostars funding. A.C.d.V. has received speaker’s fees and research grants from Janssen, Takeda, Abbvie and Tramedico. R.L.W. has received speaker’s fees and research grants from Jansen, Pfizer, and Abbvie. T.E.H.R. has received speaker’s fees from Takeda. F.D.M.v.S. has served on the advisory boards of Dr Falk, Takeda, and Galapagos. F.H. has received speaker’s fees or served on advisory boards for Abbvie, Celgene, Janssen-Cilag, MSD, Takeda, Celltrion, Teva, Sandoz and Dr Falk, and has received unrestricted grants from Dr Falk, Janssen-Cilag, Abbvie. Z.M. has received unrestricted grants from Niels Stensen Fellowship, MLDS, and Galapagos. All other authors have no conflicts of interest to declare.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
