

Viral Myocarditis Mimicking ST-Segment Elevation Myocardial Infarction Complicated by Thrombocytopenia and Vasculitic Peripheral Neuropathy
- PMID: 36433700
- PMCID: PMC9703478
- DOI: 10.1177/23247096221139271
Viral Myocarditis Mimicking ST-Segment Elevation Myocardial Infarction Complicated by Thrombocytopenia and Vasculitic Peripheral Neuropathy
Abstract
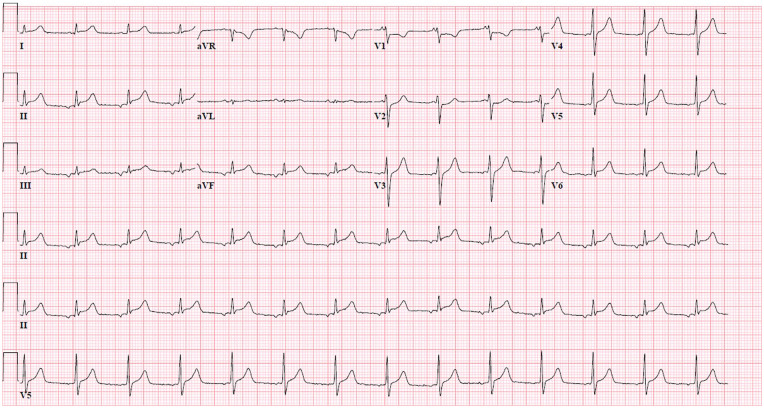
Symptomatic myocarditis is classically featured by a flu-like prodrome, dyspnea on exertion, palpitations, substernal chest pain, and abnormal electrocardiogram (ECG). The clinical diagnosis has often been challenging due to its similarities to acute coronary syndrome. Our case involved a patient who presented with claudication of bilateral lower extremity and ST-segment elevation myocardial infarction (STEMI) in the inferior leads. On cardiac catheterization, nonobstructed coronary arteries with left ventricular ejection fraction (LVEF) of 30% were demonstrated. His clinical presentation was consistent with suspected myocarditis, and he improved with immunosuppression. In addition, his thrombocytopenia and severe symptoms of peripheral neuropathy responded to both immunotherapy and anticoagulation. This case highlights the interplay between history taking, physical examination, and multimodal diagnostic imaging.
Keywords: cardiology; myocarditis; pulmonary critical care.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


Similar articles
-
Coronary artery spasm due to acute myocarditis in an adolescent: a case report.BMC Pediatr. 2022 May 24;22(1):304. doi: 10.1186/s12887-022-03354-7. BMC Pediatr. 2022. PMID: 35610586 Free PMC article.
-
A Rare Case of Myocarditis Mimicking ST-Elevation Myocardial Infarction.Cureus. 2020 Nov 24;12(11):e11671. doi: 10.7759/cureus.11671. Cureus. 2020. PMID: 33391909 Free PMC article.
-
ACUTE MYOCARDITIS IN YOUNG AGE MIMICKING AS ST-ELEVATION MYOCARDIAL INFARCTION: CASE REPORT.Georgian Med News. 2024 Mar;(348):6-9. Georgian Med News. 2024. PMID: 38807382
-
The Role of ECG in the Diagnosis and Risk Stratification of Acute Coronary Syndromes: an Old but Indispensable Tool.Curr Cardiol Rep. 2022 Feb;24(2):109-118. doi: 10.1007/s11886-021-01628-7. Epub 2022 Jan 13. Curr Cardiol Rep. 2022. PMID: 35028816 Review.
-
Electrocardiographic patterns mimicking ST segment elevation myocardial infarction.Cardiol Clin. 2012 Nov;30(4):601-15. doi: 10.1016/j.ccl.2012.07.012. Epub 2012 Oct 1. Cardiol Clin. 2012. PMID: 23102035 Review.
References
-
- Dec GW, Waldman H, Southern J, Fallon JT, Hutter AM, Palacios I. Viral myocarditis mimicking acute myocardial infarction. J AM Coll Cardiol. 1992;20:85-89. - PubMed
-
- Chow LH, Radio SJ, Sears TD, McManus BM. Insensitivity of right ventricular endomyocardial biopsy in the diagnosis of myocarditis. J Am Coll Cardiol. 1989;14:915-920. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
