

Characterization of SARS-CoV-2 antibodies in human milk from 21 women with confirmed COVID-19 infection
- PMID: 36434204
- PMCID: PMC9702863
- DOI: 10.1038/s41390-022-02360-w
Characterization of SARS-CoV-2 antibodies in human milk from 21 women with confirmed COVID-19 infection
Abstract
Background: One potential mechanism for protection from SARS-CoV-2 in children is through passive immunity via breast milk from a mother infected with the novel coronavirus. The primary objectives of this study were to establish the presence of SARS-CoV-2-specific IgA and IgG and to characterize the antigenic regions of SARS-CoV-2 proteins that were reactive with antibodies in breast milk.
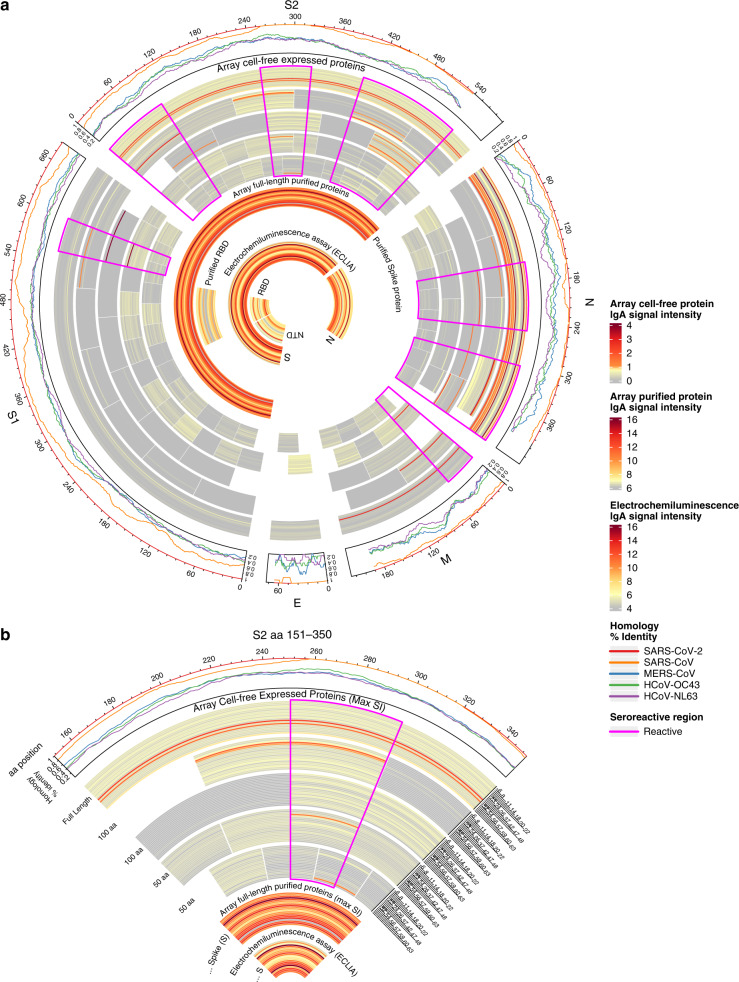
Methods: Between March 2020 and September 2020, 21 women with confirmed SARS-CoV-2 infection were enrolled in Mommy's Milk. Participants donated serial breast milk samples around their time of illness. Breast milk samples were used to probe a multi-coronavirus protein microarray containing full-length and variable-length overlapping fragments of SARS-CoV-2 proteins. Samples were also tested against S and N proteins by electrochemiluminescence assay.
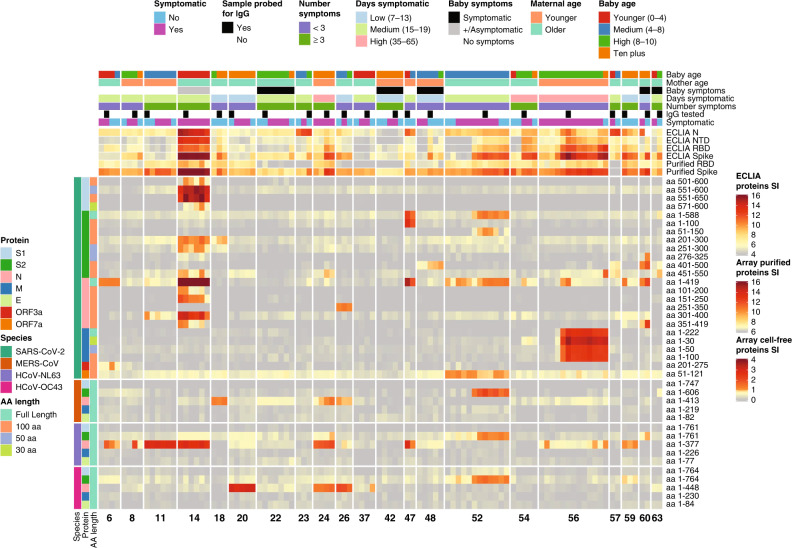
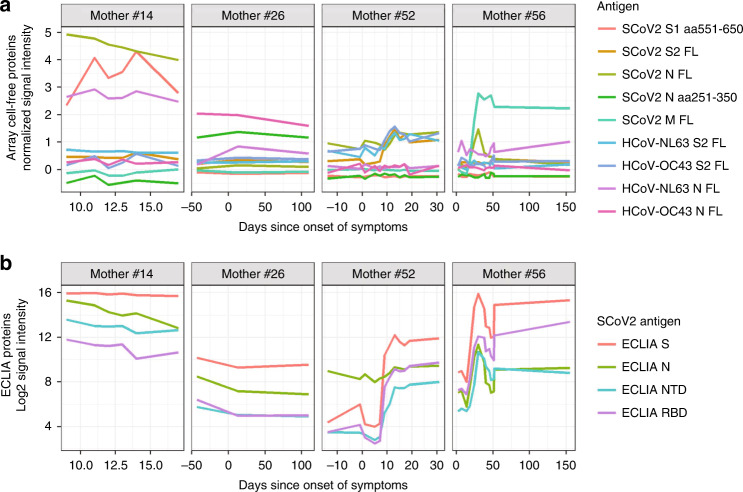
Results: The breast milk samples contained IgA reactive with a variety of SARS-CoV-2 antigens. The most IgA-reactive SARS-CoV-2 proteins were N (42.9% of women responded to ≥1 N fragment) and S proteins (23.9% responded to ≥1 fragment of S1 or S2). IgG responses were similar. A striking observation was the dissimilarity between mothers in antibody recognition, giving distinct antibody reactivity and kinetic profiles.
Conclusions: Individual COVID-19 cases had diverse and unique milk IgA profiles following the onset of symptoms.
Impact: In this observational longitudinal case series of 21 women with confirmed SARS-CoV-2 infection, IgA binding to SARS-CoV-2 proteins detected by orthologous proteome microarray and electrochemiluminescence assays was observed in >75% of women, but there was heterogeneity in which antigens and how many were reactive between women. Immunological profiles of protein regions recognized by each woman were distinct. Diverse repertoires of mucosal breast milk antibody to SARS-CoV-2 reflect heterogeneous passive transfer of maternal antibody to exposed breastfeeding infants.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Johns Hopkins University School of Medicine. COVID-19 Dashboard by the Center for System Science and Engineering (CSSE) at Johns Hopkins (accessed 4 April 2021); https://coronavirus.jhu.edu/map.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
