

Helical versus static approaches to delivering tomotherapy to the junctional target for patients taller than 135 cm undergoing total body irradiation
- PMID: 36434707
- PMCID: PMC9694876
- DOI: 10.1186/s40001-022-00886-7
Helical versus static approaches to delivering tomotherapy to the junctional target for patients taller than 135 cm undergoing total body irradiation
Abstract
Background: Helical TomoTherapy® is widely used for total body irradiation as a component of conditioning regimens before allogeneic bone-marrow transplantation. However, this technique limits the maximum length of a planning target volume to 135 cm. Therefore, patients taller than 135 cm require two planning computed tomography scans and treatment plans. The junctional target between these two treatment plans is thus a critical region for treatment planning and delivery. Here, we compare radiation coverage of the junctional target between helical and static approaches to treatment planning and delivery to determine which approach allows high quality irradiation planning and provides more robustness against patient movement.
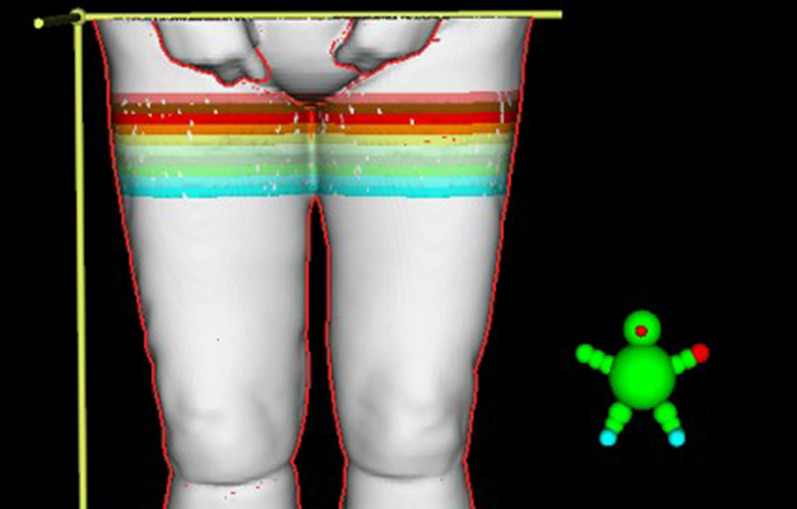
Methods: We retrospectively analyzed 10 patients who underwent total body irradiation using a static four-field box planning approach and nine patients who underwent total body irradiation using a helical planning approach. All patients were taller than 135 cm. The junctional target volume was divided into 10 slices of 1 cm thickness (JT1-JT10) for analysis. Dosimetric parameters and dose-volume histograms were compared to assess the quality of coverage of the junctional target between the helical and static planning approaches.
Results: The D50 for the total junctional target was slightly higher than the prescribed dose for both helical and static approaches, with a mean of 108.12% for the helical group and 107.81% for the static group. The mean D95 was 98.44% ± 4.19% for the helical group and 96.20% ± 4.59% for the static group. The mean homogeneity index covering the entire junctional target volume was 1.20 ± 0.04 for the helical group and 1.21 ± 0.05 for the static group. The mean homogeneity index ranged from 1.08 ± 0.01 in JT1 to 1.22 ± 0.06 in JT6 for the helical group and from 1.06 ± 0.02 in JT1 to 1.19 ± 0.05 in JT6 for the static group. There were no significant differences in parameters between helical and static groups. However, the static approach provided robustness against up to 30 mm of lateral movement of the patient.
Conclusions: As long as TBI using helical TomoTherapy® is limited to a maximum length of 135 cm, the junctional target must be addressed during treatment planning. Our analysis shows that the static four-field box approach is viable and offers higher robustness against lateral movement of the patient than the helical approach.
Keywords: Bone-marrow transplantation; Field junction; Helical tomotherapy; Overlap region; Radiotherapy; Static tomotherapy; Total body irradiation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Maeng CH, Ko YH, Lim DH, et al. Comparison of Total Body Irradiation (TBI) conditioning with non-TBI for autologous stem cell transplantation in newly diagnosed or relapsed mature T- and NK-cell non-hodgkin lymphoma. Cancer Res Treat. 2017;49(1):92–103. doi: 10.4143/crt.2015.476. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
