

Successful management of chronic urticaria and food allergies in a pediatric population using integrative traditional Chinese medicine therapy: a case series
- PMID: 36434719
- PMCID: PMC9700962
- DOI: 10.1186/s12948-022-00175-y
Successful management of chronic urticaria and food allergies in a pediatric population using integrative traditional Chinese medicine therapy: a case series
Abstract
Background: Food allergy is becoming increasingly common among the pediatric population. Despite strict avoidance of food allergens, a subgroup of sensitive individuals still develops frequent, persistent, and difficult to treat hives (FPDTH) for which there is no curative therapy. Although these cases are rare, these patients are in most need of therapy.
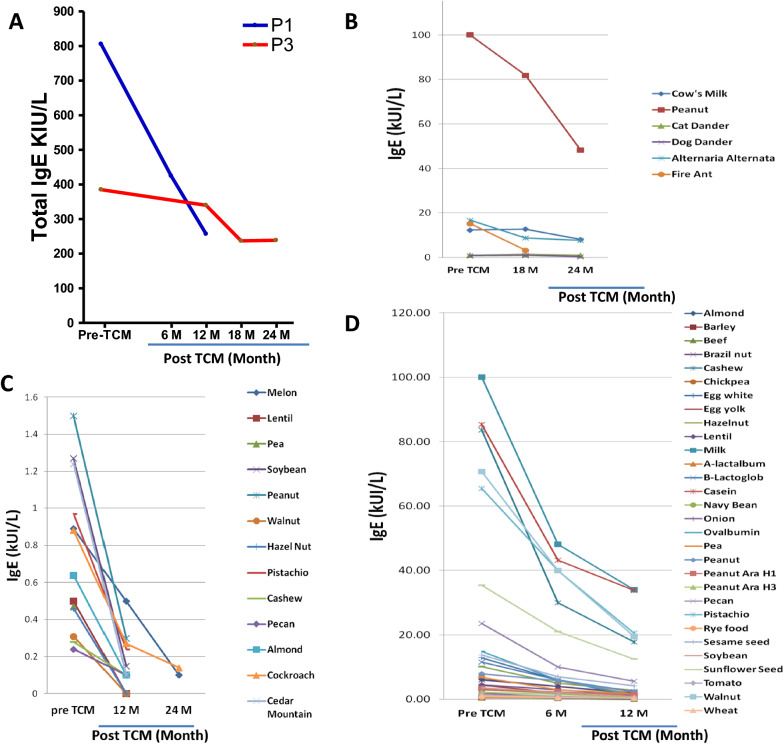
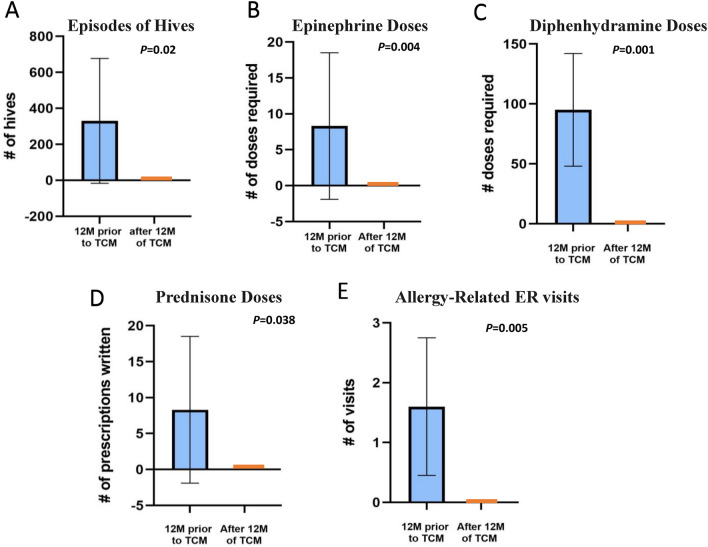
Case presentations: This is a retrospective review of 3 pediatric patients with highly sensitive food allergies who initially presented with hives daily or every other day, or multiple times a day, but achieved marked remission after traditional Chinese medicine (TCM) therapies. Patient 1 (P1) is a 5-year-old who has experienced 140 reactions in his lifetime. Reactions were mostly hives with 4 episodes of anaphylaxis. P1 had used Prednisone 20 times, had an Epinephrine injection 4 times, and had 3 emergency room (ER) visits. Patient 2 (P2) is a 12-year-old who had experienced hives since age 3. Despite daily antihistamine use, P2 had > 730 reactions in his lifetime at the time of presentation including 2 episodes of anaphylaxis. He had been prescribed prednisone 4 times, an Epinephrine injection 2 times, and had 1 ER visit. Patient 3 (P3) is a 20-month-old girl who had experienced > 120 reactions including 1 episode of anaphylaxis. She was on daily desonide and frequently used an antihistamine, yet still had required a course of prednisone once, an Epinephrine injection once, and had 1 ER visit to manage her reaction. After presenting to our clinic, patients received internal and external TCM treatments, including herbal baths and creams (Remedy A-D) as basic remedies to reduce food reactions, including but not limited to frequent hives. Within 7-9 months of TCM treatment, remarkably all patients had complete remission of atopic symptoms. All three patients also experienced an improvement in other conditions including food intolerance, diarrhea, anxiety, eczema, and environmental allergies. After 1 year of treatment, all three patients had reductions in food-specific IgE levels that had been previously elevated, and additionally, P1 and P3, who initially had high total IgE levels, experienced a marked decrease in total IgE levels as well. All three patients continued to introduce foods into their diet that they previously had reactions to, and all 3 patients remain symptom-free.
Conclusions: Three pediatric patients with a known history of multiple food sensitivities and physician-diagnosed food allergies that presented with FPDTH underwent a TCM regimen and experienced dramatic improvement in symptoms and reduction in their IgE levels. This regimen appears to be effective in FPDTH population although a further study in a controlled clinical setting is required.
Keywords: Chronic urticaria; Food allergy; Food sensitivities; Hives; IgE; Traditional Chinese medicine; Urticaria.
© 2022. The Author(s).
Conflict of interest statement
Authors Xiaowen Fan, Tory McKnight, Song Park and Johnathan Neshiwat have no conflicts of interest to disclose. Xium-Min Li and Danna Chung received practice compensation from the Integrative Health and Acupuncture PC. Both authors are part of Healthy Freedom LLC and share the patent US20160296573A1 assigned to Healthy Freedom LLC. Xiu-Min Li received additional research support from the National Institutes of Health (NIH)/National Center for Complementary and Alternative Medicine (NCCAM); Food Allergy Research and Education (FARE), Winston Wolkoff Integrative Medicine Fund for Allergies and Wellness, the Parker Foundation, and Henan University of Chinese Medicine/New York Medical College; received consultancy fees from FARE and Johnson & Johnson Pharmaceutical Research & Development, L.L.C. Bayer Global Health LLC; received royalties from UpToDate; is an Honorary Professor of Chinese Medical University, Taichung, Taiwan, and Henan University of Chinese Medicine; received travel expenses from the NCCAM, FARE and Henan University of Chinese Medicine and China Allergy Asthma College (Conference); share US patent PCT/US05/008417, PCT 14/875,772, PCT/US2014/012306, PCT/US14/68396; PCT/US2017/056822) (pending);, US Times Technology Inc is managed by the related party; is a member of Herbs Springs, LLC, Healthy Freedom LLC, and General Nutraceutical Technology.
Figures
Similar articles
-
Successful prevention of extremely frequent and severe food anaphylaxis in three children by combined traditional Chinese medicine therapy.Allergy Asthma Clin Immunol. 2014 Dec 20;10(1):66. doi: 10.1186/s13223-014-0066-5. eCollection 2014. Allergy Asthma Clin Immunol. 2014. PMID: 25670938 Free PMC article.
-
Alpha-gal syndrome initially misdiagnosed as chronic spontaneous urticaria in a pediatric patient: a case report and review of the literature.J Med Case Rep. 2023 Jan 8;17(1):6. doi: 10.1186/s13256-022-03718-8. J Med Case Rep. 2023. PMID: 36611183 Free PMC article. Review.
-
Food anaphylaxis in schools: evaluation of the management plan and the efficiency of the emergency kit.Allergy. 2001 Nov;56(11):1071-6. doi: 10.1034/j.1398-9995.2001.00047.x. Allergy. 2001. PMID: 11703221
-
Interdisciplinary Significance of Food-Related Adverse Reactions in Adulthood.Nutrients. 2020 Dec 2;12(12):3725. doi: 10.3390/nu12123725. Nutrients. 2020. PMID: 33276661 Free PMC article.
-
Traditional Chinese medicine for food allergy and eczema.Ann Allergy Asthma Immunol. 2021 Jun;126(6):639-654. doi: 10.1016/j.anai.2020.12.002. Epub 2020 Dec 10. Ann Allergy Asthma Immunol. 2021. PMID: 33310179 Review.
Cited by
-
Traditional Chinese Medicine for Pediatric Allergic Diseases.Curr Allergy Asthma Rep. 2025 Jul 31;25(1):33. doi: 10.1007/s11882-025-01208-7. Curr Allergy Asthma Rep. 2025. PMID: 40742400 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
