

Early childhood wheezing phenotypes and determinants in a South African birth cohort: longitudinal analysis of the Drakenstein Child Health Study
- PMID: 36435180
- PMCID: PMC9870786
- DOI: 10.1016/S2352-4642(22)00304-2
Early childhood wheezing phenotypes and determinants in a South African birth cohort: longitudinal analysis of the Drakenstein Child Health Study
Abstract
Background: Developmental trajectories of childhood wheezing in low-income and middle-income countries (LMICs) have not been well described. We aimed to derive longitudinal wheeze phenotypes from birth to 5 years in a South African birth cohort and compare those with phenotypes derived from a UK cohort.
Methods: We used data from the Drakenstein Child Health Study (DCHS), a longitudinal birth cohort study in a peri-urban area outside Cape Town, South Africa. Pregnant women (aged ≥18 years) were enrolled during their second trimester at two public health clinics. We followed up children from birth to 5 years to derive six multidimensional indicators of wheezing (including duration, temporal sequencing, persistence, and recurrence) and applied Partition Around Medoids clustering to derive wheeze phenotypes. We compared phenotypes with a UK cohort (the Avon Longitudinal Study of Parents and Children [ALSPAC]). We investigated associations of phenotypes with early-life exposures, including all-cause lower respiratory tract infection (LRTI) and virus-specific LRTI (respiratory syncytial virus, rhinovirus, adenovirus, influenza, and parainfluenza virus) up to age 5 years. We investigated the association of phenotypes with lung function at 6 weeks and 5 years.
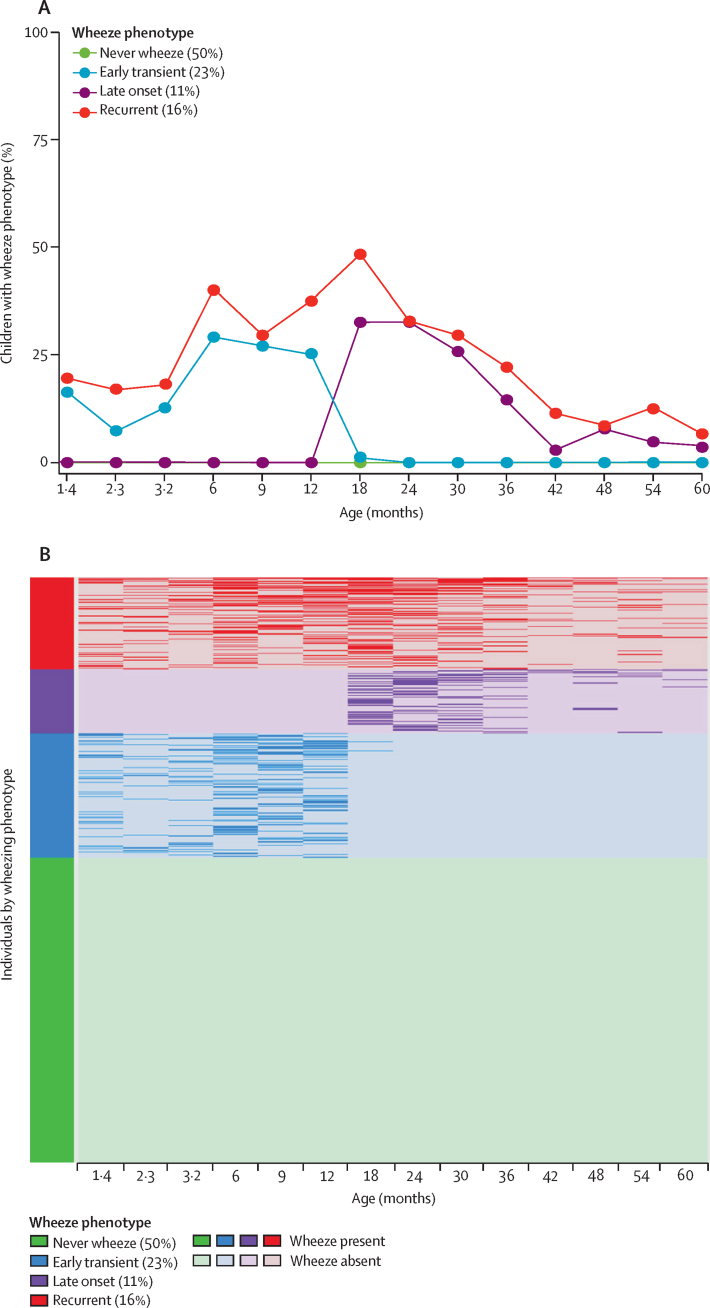
Findings: Between March 5, 2012, and March 31, 2015, we enrolled 1137 mothers and there were 1143 livebirths. Four wheeze phenotypes were identified among 950 children with complete data: never (480 children [50%]), early transient (215 children [23%]), late onset (104 children [11%]), and recurrent (151 children [16%]). Multivariate adjusted analysis indicated that LRTI and respiratory syncytial virus-LRTI, but not other respiratory viruses, were associated with increased risk of recurrent wheeze (odds ratio [OR] 2·79 [95% CI 2·05-3·81] for all LTRIs; OR 2·59 [1·30-5·15] for respiratory syncytial virus-LRTIs). Maternal smoking (1·88 [1·12-3·02]), higher socioeconomic status (2·46 [1·23-4·91]), intimate partner violence (2·01 [1·23-3·29]), and male sex (2·47 [1·50-4·04]) were also associated with recurrent wheeze. LRTI and respiratory syncytial virus-LRTI were also associated with early transient and late onset clusters. Wheezing illness architecture differed between DCHS and ALSPAC; children included in ALSPAC in the early transient cluster wheezed for a longer period before remission and late-onset wheezing started at an older age, and no persistent phenotype was identified in DCHS. At 5 years, airway resistance was higher in children with early or recurrent wheeze compared with children who had never wheezed. Airway resistance increased from 6 weeks to 5 years among children with recurrent wheeze.
Interpretation: Effective strategies to reduce maternal smoking and psychosocial stressors and new preventive interventions for respiratory syncytial virus are urgently needed to optimise child health in LMICs.
Funding: UK Medical Research Council; The Bill & Melinda Gates Foundation; National Institutes of Health Human Heredity and Health in Africa; South African Medical Research Council; Wellcome Trust.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests HJZ reports grants from the Bill & Melinda Gates Foundation, the NIH H3 Africa, the UK Medical Research council (MRC), Wellcome Trust, and the South African MRC. DG reports grants from the Wellcome Trust. AC reports personal fees from Stallergenes Greer; and personal fees from AstraZeneca, GlaxoSmithKline, and Worg Pharmaceuticals, outside the submitted work. All other authors declare no competing interests.
Figures
Similar articles
-
Early-life respiratory syncytial virus lower respiratory tract infection in a South African birth cohort: epidemiology and effect on lung health.Lancet Glob Health. 2020 Oct;8(10):e1316-e1325. doi: 10.1016/S2214-109X(20)30251-5. Lancet Glob Health. 2020. PMID: 32971054 Free PMC article.
-
Determinants of lung function development from birth to age 5 years: an interrupted time series analysis of a South African birth cohort.Lancet Child Adolesc Health. 2024 Jun;8(6):400-412. doi: 10.1016/S2352-4642(24)00072-5. Epub 2024 Apr 12. Lancet Child Adolesc Health. 2024. PMID: 38621408 Free PMC article.
-
Associations between maternal mental health and early child wheezing in a South African birth cohort.Pediatr Pulmonol. 2018 Jun;53(6):741-754. doi: 10.1002/ppul.24008. Epub 2018 Apr 10. Pediatr Pulmonol. 2018. PMID: 29635887 Free PMC article.
-
Assessing the strength of evidence for a causal effect of respiratory syncytial virus lower respiratory tract infections on subsequent wheezing illness: a systematic review and meta-analysis.Lancet Respir Med. 2020 Aug;8(8):795-806. doi: 10.1016/S2213-2600(20)30109-0. Lancet Respir Med. 2020. PMID: 32763206 Free PMC article.
-
New advances in RSV: Is prevention attainable?Pediatr Pulmonol. 2025 Mar;60 Suppl 1(Suppl 1):S120-S122. doi: 10.1002/ppul.27310. Epub 2024 Oct 28. Pediatr Pulmonol. 2025. PMID: 39466029 Free PMC article. Review.
Cited by
-
Dysfunctional neutrophil type 1 interferon responses in preschool children with recurrent wheezing and IL-4-mediated aeroallergen sensitization.J Allergy Clin Immunol Glob. 2024 Feb 13;3(2):100229. doi: 10.1016/j.jacig.2024.100229. eCollection 2024 May. J Allergy Clin Immunol Glob. 2024. PMID: 38510797 Free PMC article.
-
Patterns of Respiratory Symptoms and Asthma Diagnosis in School-Age Children: Three Birth Cohorts.Allergy. 2025 Jul;80(7):1923-1934. doi: 10.1111/all.16617. Epub 2025 Jun 12. Allergy. 2025. PMID: 40501205 Free PMC article.
-
Intra-breath changes in respiratory mechanics are sensitive to history of respiratory illness in preschool children: the SEPAGES cohort.Respir Res. 2024 Feb 24;25(1):99. doi: 10.1186/s12931-024-02701-9. Respir Res. 2024. PMID: 38402379 Free PMC article.
-
The effect of moderate-to-late preterm birth on lung function over the first 5 years of life in a South African birth cohort.ERJ Open Res. 2025 Jun 2;11(3):00733-2024. doi: 10.1183/23120541.00733-2024. eCollection 2025 May. ERJ Open Res. 2025. PMID: 40470143 Free PMC article.
-
Prenatal Factors in the Development of Allergic Diseases.Int J Mol Sci. 2024 Jun 8;25(12):6359. doi: 10.3390/ijms25126359. Int J Mol Sci. 2024. PMID: 38928067 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
