

Amplification of the PLAG-family genes-PLAGL1 and PLAGL2-is a key feature of the novel tumor type CNS embryonal tumor with PLAGL amplification
- PMID: 36437415
- PMCID: PMC9807491
- DOI: 10.1007/s00401-022-02516-2
Amplification of the PLAG-family genes-PLAGL1 and PLAGL2-is a key feature of the novel tumor type CNS embryonal tumor with PLAGL amplification
Erratum in
-
Correction to: Amplification of the PLAG-family genes-PLAGL1 and PLAGL2-is a key feature of the novel tumor type CNS embryonal tumor with PLAGL amplification.Acta Neuropathol. 2023 Apr;145(4):511-514. doi: 10.1007/s00401-023-02538-4. Acta Neuropathol. 2023. PMID: 36786841 Free PMC article. No abstract available.
Abstract
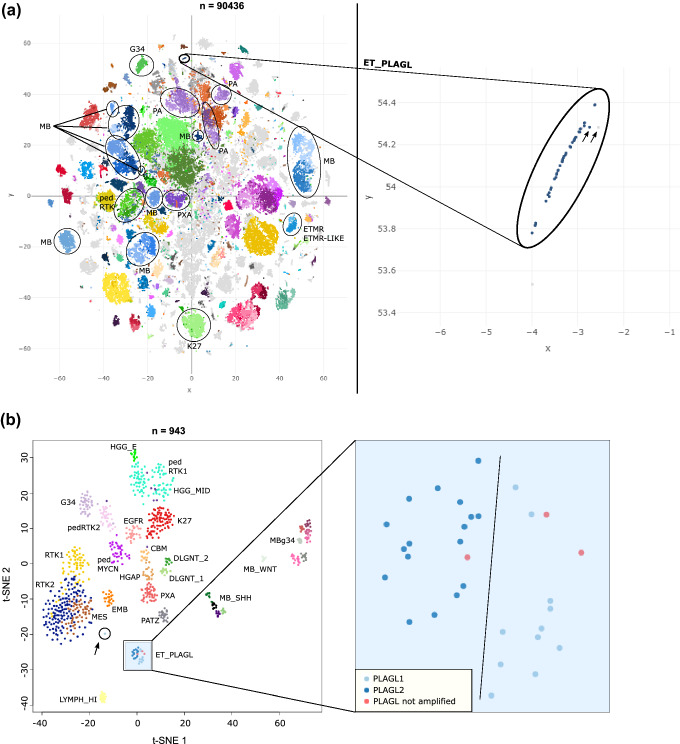
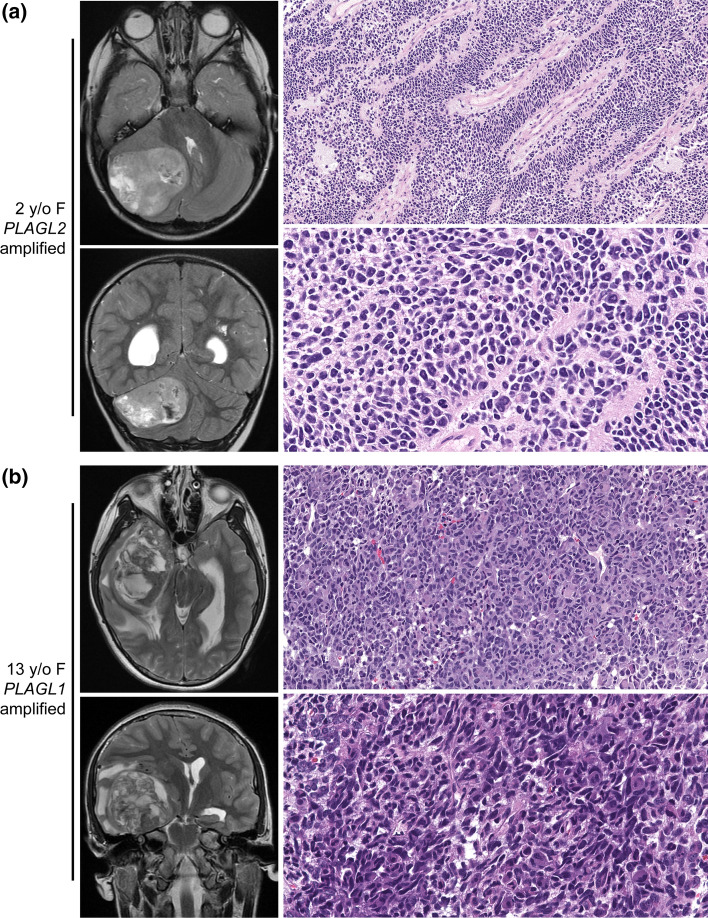
Pediatric central nervous system (CNS) tumors represent the most common cause of cancer-related death in children aged 0-14 years. They differ from their adult counterparts, showing extensive clinical and molecular heterogeneity as well as a challenging histopathological spectrum that often impairs accurate diagnosis. Here, we use DNA methylation-based CNS tumor classification in combination with copy number, RNA-seq, and ChIP-seq analysis to characterize a newly identified CNS tumor type. In addition, we report histology, patient characteristics, and survival data in this tumor type. We describe a biologically distinct pediatric CNS tumor type (n = 31 cases) that is characterized by focal high-level amplification and resultant overexpression of either PLAGL1 or PLAGL2, and an absence of recurrent genetic alterations characteristic of other pediatric CNS tumor types. Both genes act as transcription factors for a regulatory subset of imprinted genes (IGs), components of the Wnt/β-Catenin pathway, and the potential drug targets RET and CYP2W1, which are also specifically overexpressed in this tumor type. A derived PLAGL-specific gene expression signature indicates dysregulation of imprinting control and differentiation/development. These tumors occurred throughout the neuroaxis including the cerebral hemispheres, cerebellum, and brainstem, and were predominantly composed of primitive embryonal-like cells lacking robust expression of markers of glial or neuronal differentiation (e.g., GFAP, OLIG2, and synaptophysin). Tumors with PLAGL1 amplification were typically diagnosed during adolescence (median age 10.5 years), whereas those with PLAGL2 amplification were diagnosed during early childhood (median age 2 years). The 10-year overall survival was 66% for PLAGL1-amplified tumors, 25% for PLAGL2-amplified tumors, 18% for male patients, and 82% for female patients. In summary, we describe a new type of biologically distinct CNS tumor characterized by PLAGL1/2 amplification that occurs predominantly in infants and toddlers (PLAGL2) or adolescents (PLAGL1) which we consider best classified as a CNS embryonal tumor and which is associated with intermediate survival. The cell of origin and optimal treatment strategies remain to be defined.
Keywords: Molecular neuro-oncology; PLAGL1; PLAGL2; Pediatric cancer.
© 2022. The Author(s).
Conflict of interest statement
Stephen Yip is a member of advisory boards and has received honorarium from Amgen, AstraZeneca, Bayer, Incyte, and Roche. P. Wesseling, U. Schüller, A. Perry, F. Sahm, and D.A. Solomon are members of the Editorial Board of Acta Neuropathologica. They were not involved in the assessment or decision making for this manuscript.
Figures




References
-
- Central Nervous System Tumours (2021) WHO classification of tumours, 5th edition, volume 6. Edited by the WHO Classification of Tumours Editorial Board. 2021: International Agency for Research on Cancer
-
- Al Adhami H, Evano B, Le Digarcher A, Gueydan C, Dubois E, Parrinello H, et al. A systems-level approach to parental genomic imprinting: the imprinted gene network includes extracellular matrix genes and regulates cell cycle exit and differentiation. Genome Res. 2015;25(3):353–367. doi: 10.1101/gr.175919.114. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
