

Resectability of bilobar liver tumours after simultaneous portal and hepatic vein embolization versus portal vein embolization alone: meta-analysis
- PMID: 36437731
- PMCID: PMC9702575
- DOI: 10.1093/bjsopen/zrac141
Resectability of bilobar liver tumours after simultaneous portal and hepatic vein embolization versus portal vein embolization alone: meta-analysis
Abstract
Background: Many patients with bi-lobar liver tumours are not eligible for liver resection due to an insufficient future liver remnant (FLR). To reduce the risk of posthepatectomy liver failure and the primary cause of death, regenerative procedures intent to increase the FLR before surgery. The aim of this systematic review is to provide an overview of the available literature and outcomes on the effectiveness of simultaneous portal and hepatic vein embolization (PVE/HVE) versus portal vein embolization (PVE) alone.
Methods: A systematic literature search was conducted in PubMed, Web of Science, and Embase up to September 2022. The primary outcome was resectability and the secondary outcome was the FLR volume increase.
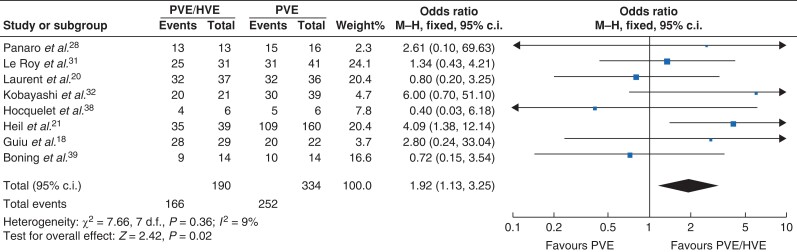
Results: Eight studies comparing PVE/HVE with PVE and six retrospective PVE/HVE case series were included. Pooled resectability within the comparative studies was 75 per cent in the PVE group (n = 252) versus 87 per cent in the PVE/HVE group (n = 166, OR 1.92 (95% c.i., 1.13-3.25)) favouring PVE/HVE (P = 0.015). After PVE, FLR hypertrophy between 12 per cent and 48 per cent (after a median of 21-30 days) was observed, whereas growth between 36 per cent and 67 per cent was reported after PVE/HVE (after a median of 17-31 days). In the comparative studies, 90-day primary cause of death was similar between groups (2.5 per cent after PVE versus 2.2 per cent after PVE/HVE), but a higher 90-day primary cause of death was reported in single-arm PVE/HVE cohort studies (6.9 per cent, 12 of 175 patients).
Conclusion: Based on moderate/weak evidence, PVE/HVE seems to increase resectability of bi-lobar liver tumours with a comparable safety profile. Additionally, PVE/HVE resulted in faster and more pronounced hypertrophy compared with PVE alone.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures

References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893–2917 - PubMed
-
- Jemal A, Bray F, Ferlay J. Global cancer statistics: 2011. CA Cancer J Clin 1999;49:33–64 - PubMed
-
- Van Cutsem E, Cervantes A, Nordlinger B, Arnold D, The ESMO Guidelines Working Group . Metastatic colorectal cancer: eSMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol. 2014;25(Suppl 3):iii1–iii9 - PubMed
-
- Cescon M, Vetrone G, Grazi GL, Ramacciato G, Ercolani G, Ravaioli Met al. . Trends in perioperative outcome after hepatic resection: analysis of 1500 consecutive unselected cases over 20 years. Ann Surg 2009;249:995–1002 - PubMed
