

Comparative efficacy of various CHIs combined with western medicine for non-small cell lung cancer: A bayesian network meta-analysis of randomized controlled trials
- PMID: 36438813
- PMCID: PMC9686447
- DOI: 10.3389/fphar.2022.1037620
Comparative efficacy of various CHIs combined with western medicine for non-small cell lung cancer: A bayesian network meta-analysis of randomized controlled trials
Abstract
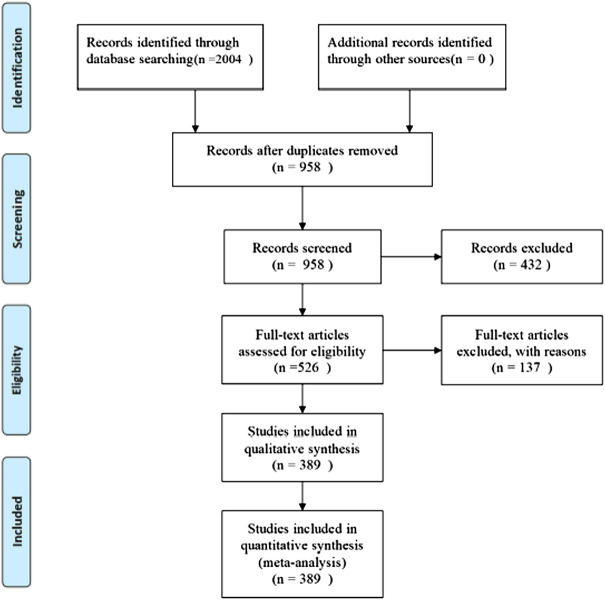
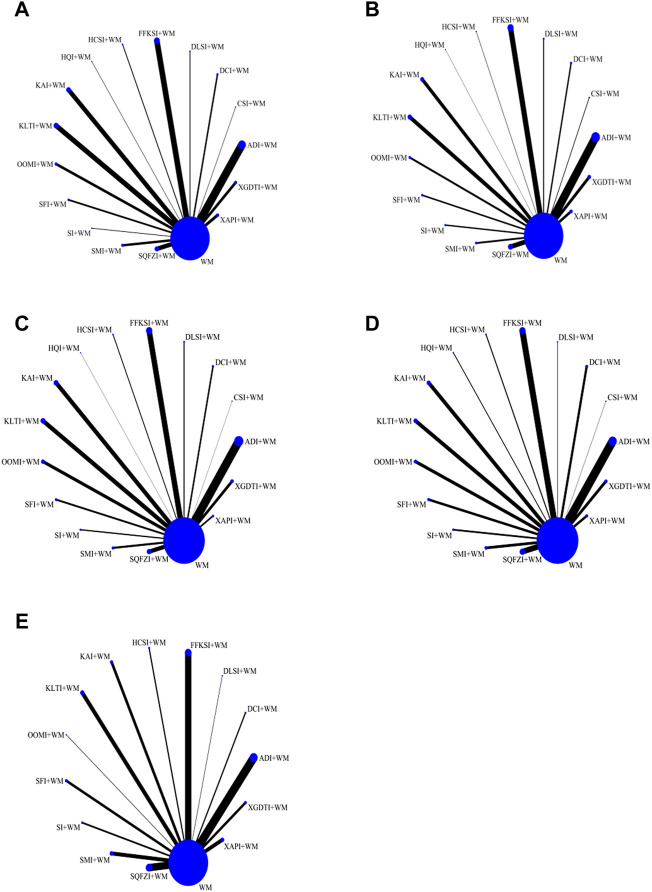
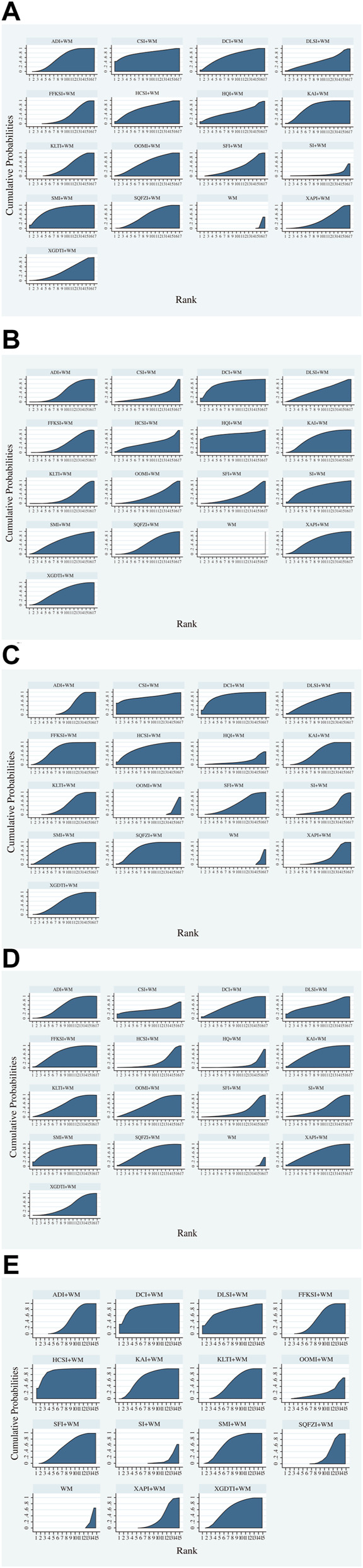
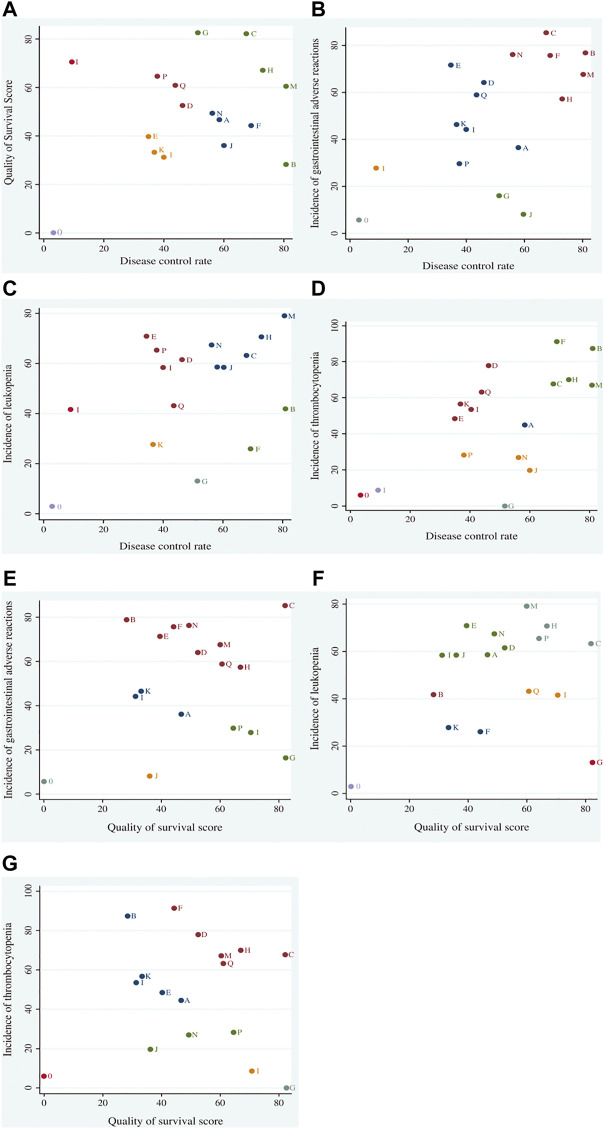
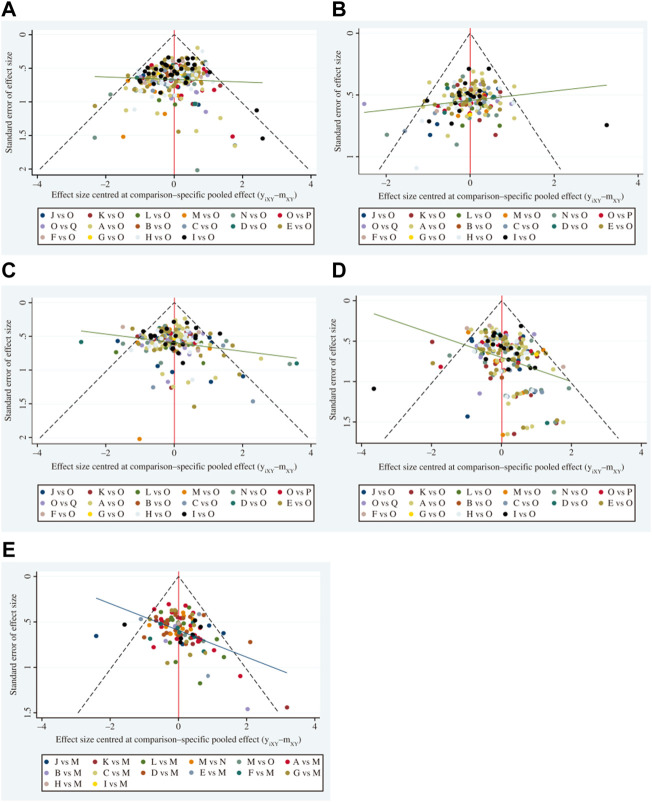
Background: Given the limitations of Western medicine (WM) for the treatment of non-small cell lung cancer (NSCLC) and the wide exploration of Chinese herbal injections (CHIs), systematically evaluate the efficacy of Various CHIs Combined with WM for Non-small Cell Lung Cancer. In this study, we performed a network meta-analysis to evaluate the comparative efficacy of 16 CHIs combined with WM regimens for the treatment of NSCLC. Methods: Literature databases were searched from their inception to November 2021, and all randomized control trials (RCTs) involving NSCLC patients treated with a combination of Chinese and WM were retrieved. Outcomes, including disease control rate, survival quality score, incidence of gastrointestinal adverse reactions, incidence of leukopenia, and incidence of thrombocytopenia, were analyzed using RevMan (5.3), Stata17, and R software. Surface under the cumulative ranking curve (SUCRA) probability values were calculated to rank the treatments examined, and clustering analysis was used to compare the effects of CHIs on different outcomes. Results: A total of 389 studies involving 31,263 patients and 16 CHIs were included. The 16 CHIs were: Aidi injection (ADI), Huachansu injection (HCSI), oil of Ophiopogon injection (OOMI), disodium cantharidinate and vitamin B6 injection (DCI), Shenfu injection (SFI), Shenmai injection (SMI), Shenqi Fuzheng injection (SQFZI), Chansu injection (CSI), Delisheng injection (DLSI), Fufang Kushen injection (FFKSI), Huangqi injection (HQI), Kangai injection (KAI), Kanglaite injection (KLTI), Shengmai injection (SI), Xiangguduotang injection (XGDTI), and Xiaoaiping injection (XAPI). The results of the network meta-analysis showed that, with WM treatment as a co-intervention, CSI was most likely to improve the disease control rate (SUCRA = 80.90%), HQI had the highest probability of being the best option for improving the survival quality score (SUCRA = 82.60%), DCI had the highest probability of reducing the incidence of gastrointestinal adverse reactions (SUCRA = 85.50%), HCSI + WM had the highest probability of reducing the incidence of thrombocytopenia (SUCRA = 91.30%), while SMI had the highest probability of reducing the incidence of leukopenia (SUCRA = 79.10%). Conclusion: CHIs combined with WM is proved to be more effective than WM alone, which may be beneficial to NSCLC patients. SMI + WM and DCI + WM are most likely the optimal CHI to improve disease control rates, survival quality score, and reduce adverse effects. This study has limitations; therefore, higher quality RCTs and real-world evidence are required to support our conclusions.
Keywords: Chinese herbal injections; Chinese medicine; bayesian model; combined therapy; network meta-analysis; non-small cell lung cancer.
Copyright © 2022 Peng, Chen, Cui, Li, Li and Peng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Efficacy of Chinese Herbal Injections for the Treatment of Primary Nephrotic Syndrome: A Bayesian Network Meta-Analysis of Randomized Controlled Trials.Front Pharmacol. 2020 Oct 16;11:579241. doi: 10.3389/fphar.2020.579241. eCollection 2020. Front Pharmacol. 2020. PMID: 33178022 Free PMC article.
-
Comparative Efficacy and Safety of Chinese Herbal Injections Combined With Cyclophosphamide and 5-Fluorouracil Chemotherapies in Treatment of Breast Cancer: A Bayesian Network Meta-Analysis.Front Pharmacol. 2021 Jan 27;11:572396. doi: 10.3389/fphar.2020.572396. eCollection 2020. Front Pharmacol. 2021. PMID: 33708106 Free PMC article.
-
Efficacy of Traditional Chinese Medicine Injection in Preventing Oxaliplatin-Induced Peripheral Neurotoxicity: An Analysis of Evidence from 3598 Patients.Evid Based Complement Alternat Med. 2022 Jul 22;2022:6875253. doi: 10.1155/2022/6875253. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 35911148 Free PMC article.
-
Comparative Efficacy of Tonic Chinese Herbal Injections for Treating Sepsis or Septic Shock: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Controlled Trials.Front Pharmacol. 2022 Mar 15;13:830030. doi: 10.3389/fphar.2022.830030. eCollection 2022. Front Pharmacol. 2022. PMID: 35370733 Free PMC article.
-
Comparative Efficacy of Chinese Herbal Injections for Treating Severe Pneumonia: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Controlled Trials.Front Pharmacol. 2022 Jan 10;12:743486. doi: 10.3389/fphar.2021.743486. eCollection 2021. Front Pharmacol. 2022. PMID: 35082663 Free PMC article. Review.
Cited by
-
Off-label use of sodium cantharidinate and vitamin B6 injection in cancer: a protocol for a systematic review and meta-analysis.Syst Rev. 2025 Apr 9;14(1):82. doi: 10.1186/s13643-025-02826-y. Syst Rev. 2025. PMID: 40205599 Free PMC article.
-
Efficacy and safety of Huachansu combined with adjuvant chemotherapy in resected colorectal cancer patients: a prospective, open-label, randomized phase II study.Med Oncol. 2023 Nov 15;40(12):358. doi: 10.1007/s12032-023-02217-0. Med Oncol. 2023. PMID: 37966546 Clinical Trial.
-
Brucea javanica Seed Oil Emulsion and Shengmai Injections Improve Peripheral Microcirculation in Treatment of Gastric Cancer.Chin J Integr Med. 2025 Apr;31(4):299-310. doi: 10.1007/s11655-024-4103-z. Epub 2024 Sep 3. Chin J Integr Med. 2025. PMID: 39225883
-
Investigating the molecular mechanisms of Fuzheng Yiliu Shenji prescription in SH-SY5Y neuroblastoma cells.Front Oncol. 2024 Sep 10;14:1447666. doi: 10.3389/fonc.2024.1447666. eCollection 2024. Front Oncol. 2024. PMID: 39319058 Free PMC article.
References
-
- Breimer L. H., Nousios P., Olsson L., Brunnstrom H. (2020). Immune checkpoint inhibitors of the PD-1/PD-L1-axis in non-small cell lung cancer: Promise, controversies and ambiguities in the novel treatment paradigm. Scand. J. Clin. Lab. Invest. 80 (5), 360–369. 10.1080/00365513.2020.1742369 - DOI - PubMed
LinkOut - more resources
Full Text Sources