

Endoscopic lumbar foraminotomy for foraminal stenosis in stable spondylolisthesis
- PMID: 36439521
- PMCID: PMC9687795
- DOI: 10.3389/fsurg.2022.1042184
Endoscopic lumbar foraminotomy for foraminal stenosis in stable spondylolisthesis
Abstract
Background: Open decompression with fusion is the gold-standard surgical technique for spondylolisthesis. However, it may be too extensive for patients with foraminal stenosis with stable spondylolisthesis. The endoscopic lumbar foraminotomy (ELF) technique was developed as a minimally invasive surgical option for foraminal stenosis. Some authors have reported the outcomes of ELF for various spondylolistheses. However, few studies have demonstrated foraminal stenosis in advanced stable spondylolisthesis. This study aimed to describe the surgical technique and results of ELF for radiculopathy due to foraminal stenosis in patients with stable spondylolisthesis.
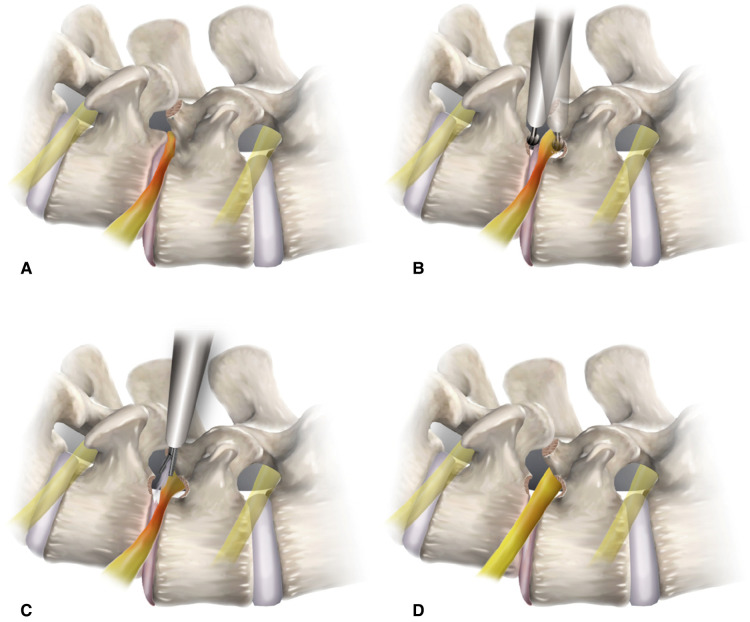
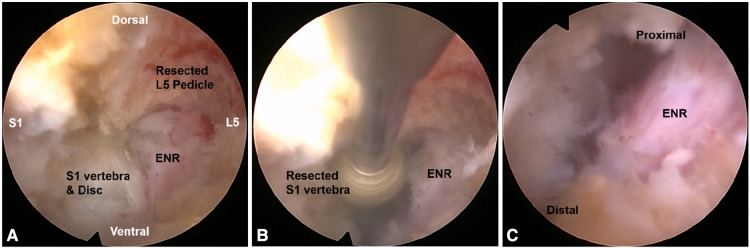
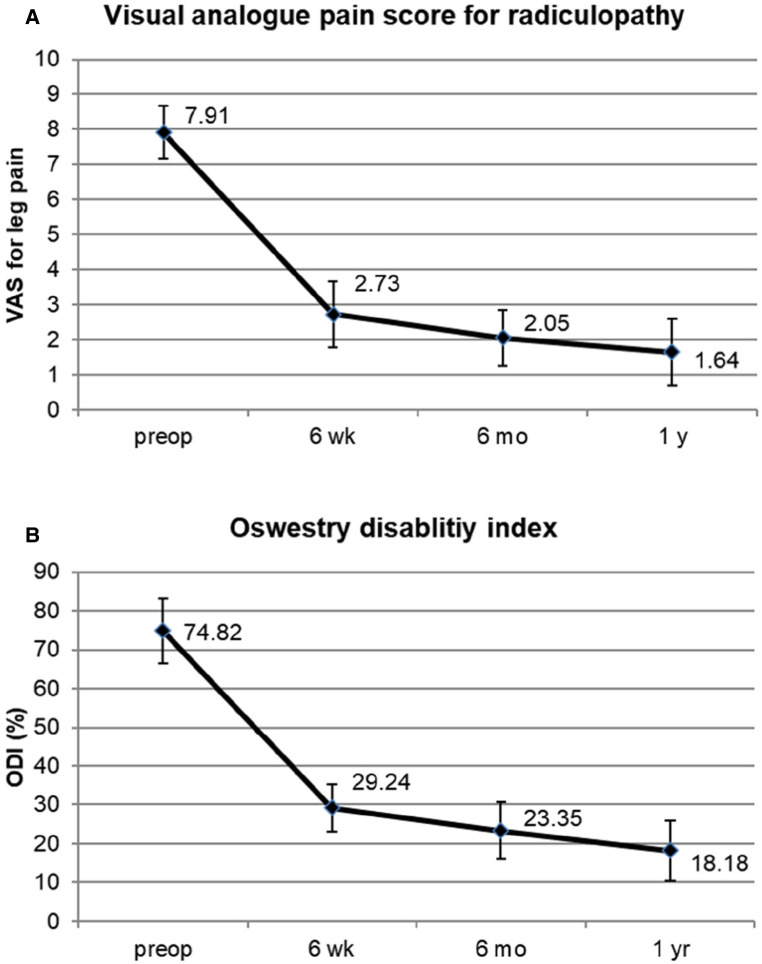
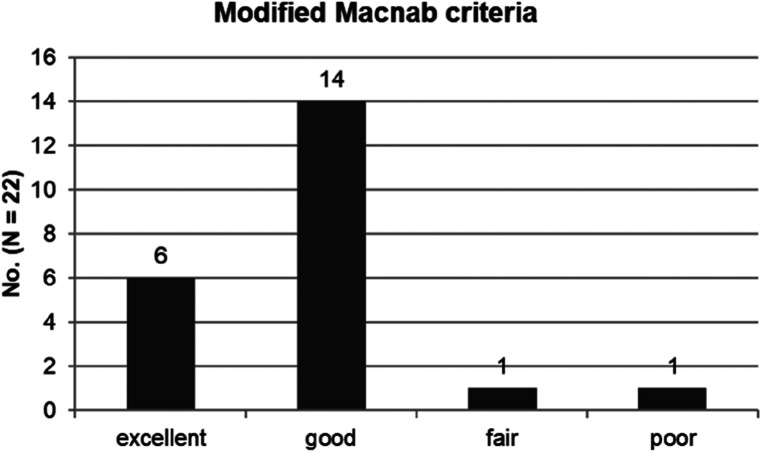
Methods: Consecutive 22 patients who suffered from radiculopathy with spondylolisthesis underwent ELF. The inclusion criterion was unilateral radicular leg pain due to foraminal stenosis in stable spondylolisthesis. After the percutaneous transforaminal approach, foraminal decompression was performed using various surgical devices under endoscopic visualization. Surgical outcomes were measured using the visual analog pain score, Oswestry disability index, and modified MacNab criteria.
Results: Pain scores and functional outcomes improved significantly during the 12-month follow-up periods. The rate of clinical improvement was 95.5% (21 of 22 patients). One patient experienced a dural tear and subsequent open surgery.
Conclusion: ELF can be effective in foraminal stenosis in stable spondylolisthesis. Technical points specializing in foraminal decompression in spondylolisthesis are required for clinical success.
Keywords: endoscopic; foraminal stenosis; foraminoplasty; foraminotomy; lumbar; percutaneous; spondylolisthesis.
© 2022 Ahn, Park, Yoo and Jeong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources