

Wingless-related integration site (WNT) signaling is activated during the inflammatory response upon cardiac surgery: A translational study
- PMID: 36440011
- PMCID: PMC9692086
- DOI: 10.3389/fcvm.2022.997350
Wingless-related integration site (WNT) signaling is activated during the inflammatory response upon cardiac surgery: A translational study
Abstract
Objective: Cardiac surgery and the use of cardiopulmonary bypass initiate a systemic inflammatory response. Wingless-related integration site (WNT) signaling is part of the innate immunity and has been attributed a major role in the regulation of inflammation. In preclinical research, WNT-5a may sustain an inflammatory response and cause endothelial dysfunction. Our aim was to investigate WNT signaling after cardiac surgery and its association with postoperative inflammation (Clinicaltrials.gov, NCT04058496).
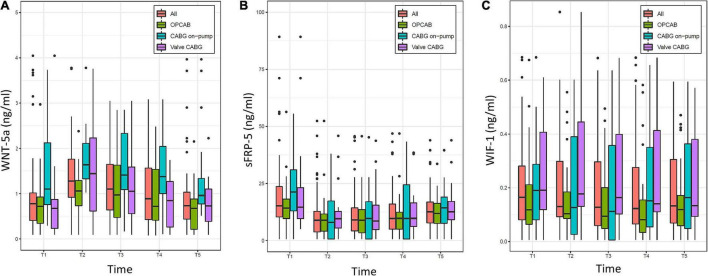
Methods: In this prospective, single-center, observational study, 64 consecutive patients for coronary artery bypass grafting (CABG) ± valve surgery were assigned into three groups: off-pump CABG (n = 28), on-pump CABG (n = 16) and combined valve-CABG surgery (n = 20). Blood samples were acquired before surgery, at intensive care unit (ICU) admission and 4, 8, and 48 h thereafter. Plasma concentrations of WNT-5a and its antagonists Secreted frizzled-related protein 1 (sFRP-1), Secreted frizzled-related protein 5 (sFRP-5), and WNT inhibitory factor 1 (WIF-1) were determined by enzyme-linked immunosorbent assay. In addition, plasma concentrations of six inflammatory cytokines were measured by multiplex immunoassay. Parameters were analyzed for evolution of plasma concentration over time, interactions, intergroup differences, and association with clinical outcome parameters.
Results: At baseline, WNT-5a, sFRP-1, and WIF-1 were present in a minimal concentration, while sFRP-5 was elevated. A higher baseline value of WNT-5a, sFRP-5, and WIF-1 resulted in higher subsequent values of the respective parameter. At ICU admission, WNT-5a and sFRP-5 reached their maximum and minimum value, respectively. WIF-1 decreased over time and was lowest 8 h after surgery. sFRP-1 changed minimally over time. While WNT-5a returned to the baseline within 48 h, sFRP-5 and WIF-1 did not reach their baseline value at 48 h. Of the investigated WNT system components, only WIF-1 partially reflected the severity of surgery. WNT-5a and WIF-1 had an impact on postoperative fluid balance and noradrenaline requirement.
Conclusion: WNT-5a, sFRP-5, and WIF-1 are part of the systemic inflammatory response after cardiac surgery. WNT-5a peaks immediately after cardiac surgery and returns to baseline within 48 h, presumably modulated by its antagonist sFRP-5. Based on this translational study, WNT-5a antagonism may be further investigated to assess potentially beneficial effects in patients with a dysregulated inflammation after cardiac surgery.
Keywords: SIRS; WNT signaling; WNT-5a; cardiac surgery; cardiopulmonary bypass; inflammation; inflammatory biomarkers; systemic inflammatory response syndrome.
Copyright © 2022 Krüger, Hofer, Rudiger, Spahn, Braun, Bettex, Schoedon and Spahn.
Conflict of interest statement
The academic department of author DS has received grant support from Vifor SA and Vifor (International) AG. DS is co-chair of the ABC-Trauma Faculty, sponsored by unrestricted educational grants from Novo Nordisk Health Care AG, CSL Behring GmbH, LFB Biomédicaments, and Octapharma AG. DS received honoraria/travel support for consulting or lecturing from Alexion Pharmaceuticals Inc., AstraZeneca AG, Bayer AG, B. Braun Melsungen AG, CSL Behring GmbH, Celgene International II Sàrl, Daiichi Sankyo AG, Haemonetics, Instrumentation Laboratory (Werfen), LFB Biomédicaments, Merck Sharp & Dohme, Novo Nordisk Health Care AG, PAION Deutschland GmbH, Pharmacosmos A/S, Pfizer AG, Pierre Fabre Pharma, Portola Schweiz GmbH, Roche Diagnostics International Ltd, Sarstedt AG & Co., Shire Switzerland GmbH, Takeda, Tem International GmbH, Vifor Pharma, Vifor (International) AG, and Zuellig Pharma Holdings. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Glucocorticoid therapy suppresses Wnt signaling by reducing the ratio of serum Wnt3a to Wnt inhibitors, sFRP-1 and Wif-1.Clin Rheumatol. 2021 Jul;40(7):2947-2954. doi: 10.1007/s10067-020-05554-x. Epub 2021 Jan 9. Clin Rheumatol. 2021. PMID: 33420868
-
The key role of proinflammatory cytokines, matrix proteins, RANKL/OPG and Wnt/β-catenin in bone healing of hip arthroplasty patients.Bone. 2018 Feb;107:66-77. doi: 10.1016/j.bone.2017.11.004. Epub 2017 Nov 10. Bone. 2018. PMID: 29129760
-
WNT pathway in oral cancer: epigenetic inactivation of WNT-inhibitors.Oncol Rep. 2010 Oct;24(4):1035-41. doi: 10.3892/or.2010.1035. Oncol Rep. 2010. PMID: 20811686
-
The Wnt antagonist and secreted frizzled-related protein 5: implications on lipid metabolism, inflammation, and type 2 diabetes mellitus.Biosci Rep. 2018 Jul 2;38(4):BSR20180011. doi: 10.1042/BSR20180011. Print 2018 Aug 31. Biosci Rep. 2018. PMID: 29789397 Free PMC article. Review.
-
Secreted frizzled related proteins: Implications in cancers.Biochim Biophys Acta. 2014 Jan;1845(1):53-65. doi: 10.1016/j.bbcan.2013.11.004. Epub 2013 Dec 5. Biochim Biophys Acta. 2014. PMID: 24316024 Review.
Cited by
-
Effect of Continuous Intraoperative Dexmedetomidine on Interleukin-6 and Other Inflammatory Markers After Coronary Artery Bypass Graft Surgery: A Randomized Controlled Trial.Medicina (Kaunas). 2025 Apr 24;61(5):787. doi: 10.3390/medicina61050787. Medicina (Kaunas). 2025. PMID: 40428745 Free PMC article. Clinical Trial.
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials