

Markers of cell death predict therapy response in patients with cirrhosis and hepatorenal syndrome
- PMID: 36441143
- PMCID: PMC9892429
- DOI: 10.1002/ueg2.12337
Markers of cell death predict therapy response in patients with cirrhosis and hepatorenal syndrome
Abstract
Background and aims: Hepatorenal syndrome is a major complication in patients with cirrhosis and associated with high mortality. Predictive biomarkers for therapy response are largely missing. Cytokeratin18-based cell death markers are significantly elevated in patients with complications of chronic liver disease, but the role of these markers in patients with HRS treated with vasoconstrictors and albumin is unknown.
Methods: We prospectively analyzed a total of 138 patients with HRS, liver cirrhosis without HRS and acute kidney injury treated at the University Medical Center Mainz between April 2013 and July 2018. Serum levels of M30 and M65 were analyzed by ELISA and clinical data were collected. Predictive ability was assessed by Kaplan-Meier curves, logistic regression and c-statistic. Primary endpoint was response to therapy.
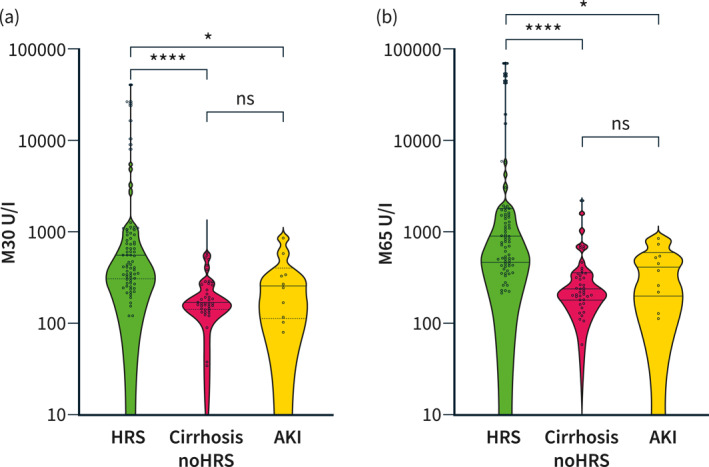
Results: M30 and M65 were significantly increased in patients with HRS compared to non-HRS controls (M30: p < 0.0001; M65: p < 0.0001). Both serum markers showed predictive ability for dialysis- and LTX-free survival but not overall survival. Logistic regression confirmed M30 and M65 as independent prognostic factors for response to therapy. A novel predictive score comprising bilirubin and M65 showed highest predictive ability to predict therapy response.
Conclusions: Serum levels of M30 and M65 can robustly discriminate patients into responders and non-responders to terlipressin therapy with a good predictive ability for dialysis- and LTX-free survival in cirrhotic patients. Cell death parameters might possess clinical relevance in patients with liver cirrhosis and HRS.
Keywords: cytokeratin-18; hepatorenal syndrome; terlipressin; therapy response.
© 2022 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC. on behalf of United European Gastroenterology.
Conflict of interest statement
There are no conflicts of interest for all authors.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
