

Continuous prolonged prone positioning in COVID-19-related ARDS: a multicenter cohort study from Chile
- PMID: 36441352
- PMCID: PMC9702866
- DOI: 10.1186/s13613-022-01082-w
Continuous prolonged prone positioning in COVID-19-related ARDS: a multicenter cohort study from Chile
Abstract
Background: Prone positioning is currently applied in time-limited daily sessions up to 24 h which determines that most patients require several sessions. Although longer prone sessions have been reported, there is scarce evidence about the feasibility and safety of such approach. We analyzed feasibility and safety of a continuous prolonged prone positioning strategy implemented nationwide, in a large cohort of COVID-19 patients in Chile.
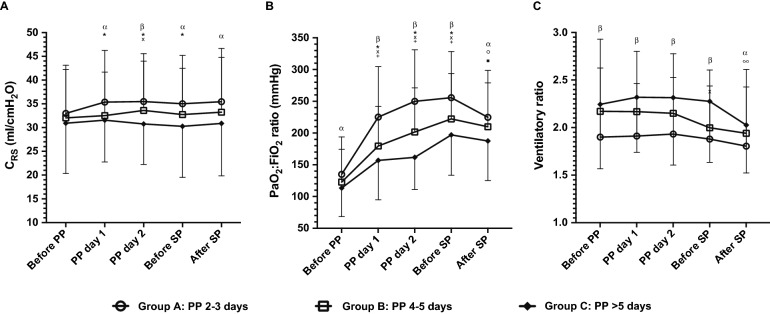
Methods: Retrospective cohort study of mechanically ventilated COVID-19 patients with moderate-to-severe acute respiratory distress syndrome (ARDS), conducted in 15 Intensive Care Units, which adhered to a national protocol of continuous prone sessions ≥ 48 h and until PaO2:FiO2 increased above 200 mm Hg. The number and extension of prone sessions were registered, along with relevant physiologic data and adverse events related to prone positioning. The cohort was stratified according to the first prone session duration: Group A, 2-3 days; Group B, 4-5 days; and Group C, > 5 days. Multivariable regression analyses were performed to assess whether the duration of prone sessions could impact safety.
Results: We included 417 patients who required a first prone session of 4 (3-5) days, of whom 318 (76.3%) received only one session. During the first prone session the main adverse event was grade 1-2 pressure sores in 97 (23.9%) patients; severe adverse events were infrequent with 17 non-scheduled extubations (4.2%). 90-day mortality was 36.2%. Ninety-eight patients (24%) were classified as group C; they exhibited a more severe ARDS at baseline, as reflected by lower PaO2:FiO2 ratio and higher ventilatory ratio, and had a higher rate of pressure sores (44%) and higher 90-day mortality (48%). However, after adjustment for severity and several relevant confounders, prone session duration was not associated with mortality or pressure sores.
Conclusions: Nationwide implementation of a continuous prolonged prone positioning strategy for COVID-19 ARDS patients was feasible. Minor pressure sores were frequent but within the ranges previously described, while severe adverse events were infrequent. The duration of prone session did not have an adverse effect on safety.
Keywords: Acute respiratory distress syndrome; Coronavirus disease 2019; Mechanical ventilation; Prone positioning.
© 2022. The Author(s).
Conflict of interest statement
RC reports grant from the National Fund for Scientific and Technological Development (FONDECYT) of the Government of Chile (1161510). No other disclosures were reported.
Figures
References
-
- Guérin C, Beuret P, Constantin JM, Bellani G, Garcia-Olivares P, Roca O, et al. A prospective international observational prevalence study on prone positioning of ARDS patients: the APRONET (ARDS Prone Position Network) study. Intensive Care Med. 2018;44(1):22–37. doi: 10.1007/s00134-017-4996-5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
