

Autoimmune Encephalitis Misdiagnosis in Adults
- PMID: 36441519
- PMCID: PMC9706400
- DOI: 10.1001/jamaneurol.2022.4251
Autoimmune Encephalitis Misdiagnosis in Adults
Abstract
Importance: Autoimmune encephalitis misdiagnosis can lead to harm.
Objective: To determine the diseases misdiagnosed as autoimmune encephalitis and potential reasons for misdiagnosis.
Design, setting, and participants: This retrospective multicenter study took place from January 1, 2014, to December 31, 2020, at autoimmune encephalitis subspecialty outpatient clinics including Mayo Clinic (n = 44), University of Oxford (n = 18), University of Texas Southwestern (n = 18), University of California, San Francisco (n = 17), University of Washington in St Louis (n = 6), and University of Utah (n = 4). Inclusion criteria were adults (age ≥18 years) with a prior autoimmune encephalitis diagnosis at a participating center or other medical facility and a subsequent alternative diagnosis at a participating center. A total of 393 patients were referred with an autoimmune encephalitis diagnosis, and of those, 286 patients with true autoimmune encephalitis were excluded.
Main outcomes and measures: Data were collected on clinical features, investigations, fulfillment of autoimmune encephalitis criteria, alternative diagnoses, potential contributors to misdiagnosis, and immunotherapy adverse reactions.
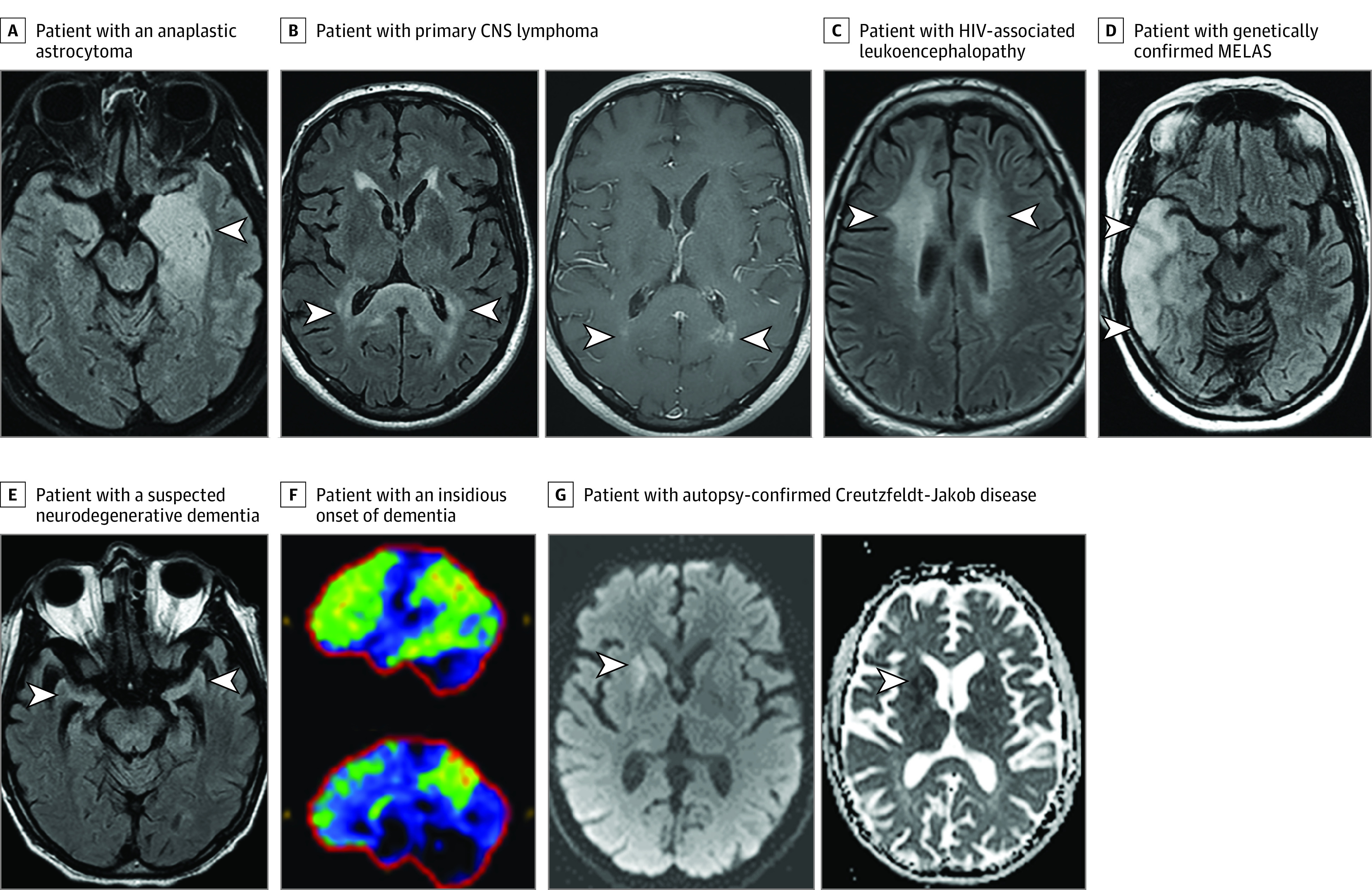
Results: A total of 107 patients were misdiagnosed with autoimmune encephalitis, and 77 (72%) did not fulfill diagnostic criteria for autoimmune encephalitis. The median (IQR) age was 48 (35.5-60.5) years and 65 (61%) were female. Correct diagnoses included functional neurologic disorder (27 [25%]), neurodegenerative disease (22 [20.5%]), primary psychiatric disease (19 [18%]), cognitive deficits from comorbidities (11 [10%]), cerebral neoplasm (10 [9.5%]), and other (18 [17%]). Onset was acute/subacute in 56 (52%) or insidious (>3 months) in 51 (48%). Magnetic resonance imaging of the brain was suggestive of encephalitis in 19 of 104 patients (18%) and cerebrospinal fluid (CSF) pleocytosis occurred in 16 of 84 patients (19%). Thyroid peroxidase antibodies were elevated in 24 of 62 patients (39%). Positive neural autoantibodies were more frequent in serum than CSF (48 of 105 [46%] vs 7 of 91 [8%]) and included 1 or more of GAD65 (n = 14), voltage-gated potassium channel complex (LGI1 and CASPR2 negative) (n = 10), N-methyl-d-aspartate receptor by cell-based assay only (n = 10; 6 negative in CSF), and other (n = 18). Adverse reactions from immunotherapies occurred in 17 of 84 patients (20%). Potential contributors to misdiagnosis included overinterpretation of positive serum antibodies (53 [50%]), misinterpretation of functional/psychiatric, or nonspecific cognitive dysfunction as encephalopathy (41 [38%]).
Conclusions and relevance: When evaluating for autoimmune encephalitis, a broad differential diagnosis should be considered and misdiagnosis occurs in many settings including at specialized centers. In this study, red flags suggesting alternative diagnoses included an insidious onset, positive nonspecific serum antibody, and failure to fulfill autoimmune encephalitis diagnostic criteria. Autoimmune encephalitis misdiagnosis leads to morbidity from unnecessary immunotherapies and delayed treatment of the correct diagnosis.
Conflict of interest statement
Figures
Comment in
-
Autoimmune Encephalitis-Misdiagnosis, Misconceptions, and How to Avoid Them.JAMA Neurol. 2023 Jan 1;80(1):12-14. doi: 10.1001/jamaneurol.2022.4154. JAMA Neurol. 2023. PMID: 36441535 No abstract available.
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
